The anti-mask, anti-vaccine clamor is destroying the United States. We need not repeat the disastrous cataclysms of the past.
Although pseudoscience may be literally defined as “false” science, it is much more. It grows out of the need to promote and popularize a myth which is accepted based on some authoritarian view or bias, religious, political, or philosophical, and the need to justify that view with “facts” which are carefully selected to support the view and presented in a way to mimic the scientific method.”— The Black Dragon Trilogy by JOHNATHAN KIEL https://a.co/hnHWBsg. This kind of propaganda now depends on the internet and social media full of testimonials and posting unsubstantiated reports supporting the emotional assertions. Testimonials are not science and neither are uncontrolled observations leading to causal conclusions based on association, especially time related causality. This is not science. It is not based on the scientific method. People also confuse the unedited collection of adverse reactions data by the FDA on medicines and vaccines as causal proof, but it is only to consider all possible adverse reactions for future rigorous scientific investigation using the scientific method (https://www.fda.gov/files/vaccines,%20blood%20&%20biologics/published/Understanding-the-Vaccine-Adverse-Event-Reporting-System-(VAERS).pdf. and https://www.nature.com/articles/d41586-021-00290-x?utm_source=Nature+Briefing&utm_campaign=5eb3714930-briefing-dy-20210217&utm_medium=email&utm_term=0_c9dfd39373-5eb3714930-43804265).
The most notorious example of pseudoscience perpetrated by a scientist involved AIDS in South Africa. UC Berkeley professor Dr. Peter Duesberg, a University of California at Berkeley, tenured professor in the Department of Molecular and Cell Biology, believed that HIV does not cause AIDS. In 1987, he first questioned the link between HIV and AIDS in the journal Cancer Research (“Retroviruses as carcinogens and pathogens: Expectations and reality”. Cancer Research 47 (5): 1199–220, 1987).” In 2000, Duesberg was a prominent member of the panel which advised President Thabo Mbeki of South Africa on the cause of the AIDS epidemic which was exploding out of control in South Africa. This “scientific support” led President Mbeki to deny AIDS was caused by a virus and denied anti-viral treatments in his country. Between 2000 and 2005, more than 330,000 deaths and an estimated 35,000 infant HIV infections occurred. Nicoli Nattrass of the University of Cape Town estimated 343,000 additional AIDS-related deaths and 171,000 infections occurred because of President Mbeki’s administration’s policies. According to Peter Mandelson in 2002, a British Labour Party politician and President of the international think tank Policy Network, it was a “genocide by sloth”. Duesberg recently still asserted his views in a paper first published in 2009, then withdrawn and republished in a revised form, in the peer-reviewed journal The Italian Journal of Anatomy and Embryology (IJAE) in December 2011. This example shows that scientists can also be lured into supporting pseudoscience if they do not manage their biases and remain true to the scientific method even when it contradicts their most favorite hypotheses (I did not say “theories”, which are often confused with the term “theoretical”). Scientific hypotheses are just that, they remain to be tested with well-designed experimentation, while scientific theories, like evolution, or the theory of relativity, are supported by many generations of observations and experimentation and predictive science before being generally accepted as a scientific consensus.
In respect to vaccination hesitancy and resistance, the consequences can be swift and devastating, with diseases almost never seen anymore, erupting abruptly seemingly out of nowhere. From 2011 to date, measles has become a problem for public health officials in the US. There were 220 cases in 2011, just 55 in 2012 and 186 in 2013. The illnesses have appeared in clusters for the most part, although single cases have also appeared in many states. In 2014, there have been three large measles outbreaks. Southern California saw an outbreak from January through May 2014 at 59 cases. New York City had an outbreak that stopped at 26 cases. Ohio has had an outbreak through 16 May 2014, with 83 people infected In 2013 through 2014, in the US, three outbreaks accounted for most of the measles cases. These included clusters of measles cases: in Texas tied to the Kenneth Copeland televangelism ministry and his mega-church; in North Carolina linked to a Hindu religious community and shrine; and in New York City, in 2014, in the Hasidic Orthodox Jewish community in Brooklyn. The national measles report from the Centers for Disease Control 1 Jan through 9 May 2014, released 12 May 2014, showed 187 measles cases from 17 states. Since that report, Ohio reported an additional 23 cases, with new cases in Tennessee, Pennsylvania, Massachusetts, and other states. The measles cases in both Ohio and California, in 2014, were linked to an ongoing measles epidemic in the Philippines. Both outbreaks in the States were results of travelers returning from the Philippines who had not been vaccinated and who brought back incubating measles. Six cases in Washington State were in patients without immunizations with ties to the Dutch Reformed Church, in British Columbia, which was the center of a 400-case outbreak of measles. The church opposes the use of all vaccines, including the measles vaccine. These examples illustrate the effects of misinformation, particularly on the internet and social media, where its removal is problematic, and perhaps, where it remains eternal. A study of the correlation of the dissemination of such information, the decline of vaccination, and the occurrence of cases should be made. My hypothesis is that the correlation would be high, and the pattern would resemble the spread of an infectious disease itself, with the computer being the vector and the electronic misinformation being the infectious agent (at least a surrogate for measles). Now imagine the consequences of anti-vaccination campaigns against SARS-CoV-2 and the devastation which has already occurred at this writing to date, continuing indefinitely because herd immunity can never be reached through “natural means” and large populations of unfettered virus allows for probable continuous emergence and “ natural selection” of resistant variants. This is, as I have posted earlier, the common nature of coronaviruses. Finally, as noted in a previous post, development of immunity after widespread dissemination of the virus in organs and tissues sets them up for devastating immune mediated complement interactions and innate immune cell (neutrophil and other granulocyte) mediated collateral destruction of blood vessels and other tissues.
All this being said, potential detrimental effects as well as beneficial ones of treatments and vaccines must be reported and investigated by the scientific method with even handedness. This includes herbal and indigenous peoples’ remedies. Historically, pharmaceuticals and pharmacology are deeply rooted in botany of medicinal plants; many which originated in folk remedies but which stood scientific scrutiny. Examples include Belladona (resulted in atropine and scopolamine), digitalis (digoxin), quinine, and lastly, the very important antimalarial drug Artemisinin (Chinese remedy). Belladonna (Atropa belladonna) is a plant which has been used as a medicine since ancient times. “Belladonna” means “beautiful women” used by the ladies of Renaissance Italy to enlarge their pupils, which they found alluring. But because it can be a lethal poison, the plant of origin also goes by the more sinister name deadly nightshade. Digoxin and digitalis are cardiac glycosides derived from the plant, foxglove, used to treat mild to moderate congestive heart failure and abnormally rapid atrial rhythms (atrial fibrillation, atrial flutter, and atrial tachycardia). The quinine mentioned above, and its present day Chinese successor, Artemisinin (from Wormwood), are actually very old remedies. Quinine, from the bark of the cinchona tree, and which can now be made synthetically, was originally discovered by the Quechua, indigenous people of Peru and Bolivia. Jesuit Missionaries were the first to introduce cinchona to Europe in the 17th century. Chinese herbalist’s use of Artemisia annua (Wormwood), which predated quinine, was first described in a 4th-century Chinese text, the source of the modern day antimalarial drug arteminisin. Quinine was commonly used for treatment of malaria until the 1940s, when chloroquine and other drugs were developed because they had fewer side effects. Except for vitamin D3 (addressed in a previous post) and some ongoing studies on the microbiome, I know of no other natural remedies being scientifically examined for prevention or treatment of COVID at this time. However, recent studies don’t support the expectations for Vitamin D3. In a study of hospitalized COVID-19 patients, a single high dose of vitamin D3 did not significantly shorten hospital lengths of stay. These findings do not support the use of high dose vitamin D3 for treatment of moderate to severe COVID-19. Criticism of this study suggesting that it did not look at subpopulations of different severity independently or early treatment suggests that the treatment should not be rejected before it has been further studied and then found effective or not (https://jamanetwork.com/journals/jama/articlepdf/2776738/jama_murai_2021_oi_200145_1613509376.92008.pdf and https://jamanetwork.com/journals/jama/articlepdf/2776736/to jama_leaf_2021_ed_200126_1613509372.9982.pdf). Vaccination, in spite of variants, (https://www.researchsquare.com/article/rs-226857/v1 and https://jamanetwork.com/journals/jama/articlepdf/2776739/jama_walensky_2021_vp_210031_1613509382.71695.pdf.) and sanitary precautions are still our best defense against COVID. What is certain, COVID can be lethal and can have persistent long term debilitating effects which are lacking with vaccination and can be prevented by it.
With the reported rise of mutants with increased transmissibility and potential immune escape supported by epidemiological and clinical data, the search for a panacea which will cover all strains of SARS-CoV-2 has become a frenzied pursuit. Such haste and grasping any favorable observations, no matter how tenuous, have inundated social media, the press, and placed undue pressure on medical institutions to modify and scale back their warnings about such unsubstantiated treatments and prophylactics, https://www.nytimes.com/interactive/2021/health/coronavirus-mutations-B117-variant.html. The problem is balancing the specific with the non-specific. The former decreases adverse side effects, such as anaphylaxis and Guillain-Barré syndrome (GBS; neurological weakness and paralysis), but is subject to mutation leading to neutralization of effectiveness. The 1976 flu vaccine, I took while in the military and which was falsely associated with GBS, rose public concern and misconceptions and fears because of a historic small increase in GBS risk associated with the vaccine, which was later found to be lower than initially thought. Concerns about vaccine-related GBS risk persist despite comprehensive surveillance of influenza vaccine-related increases showing only one additional case of GBS per million flu vaccinations. In contrast, the risk of flu-related complications is 17 per million cases. A recent study showed no link between COVID-19 and Guillain-Barré syndrome https://www.cidrap.umn.edu/news-perspective/2020/12/study-finds-no-link-between-covid-19-guillain-barr-syndrome and https://academic.oup.com/brain/advance-article/doi/10.1093/brain/awaa433/6031905. The most common trigger for GBS is infection with Campylobacter jejuni, a bacterium that causes gastroenteritis, or infection of the digestive tract, the most common cause of food borne illness. Therefore, benefits of vaccination far outweigh the risks. The use of broad spectrum, non-specific potential treatments have more adverse side effects associated with them, and diluted effectiveness.
What are we up against? Three mutants V367F, W436R, and D364Y, have arisen in Wuhan, Shenzhen, Hong Kong, and France, which have demonstrated higher human ACE2 affinity. This is because of enhanced stabilization of the receptor binding protein (receptor binding domain, RBD). High frequencies of RBD mutations have been identified: V367F with five mutations from France and one Hong Kong mutant, V483A, and G476S mutant from the USA. Lineage B.1.1.7 (also called 501Y.V1) is rapidly spreading in southeastern England. It has 17 mutations which developed prior to its detection in early September 2020, which indicates prior evolution, possibly in a chronically infected patient. B.1.1.7 expanded when SARS-CoV-2 cases were widespread and achieved dominance by outcompeting an existing population of circulating virus, natural selection of virus more transmissible. Dr. Joel Ernst, an infectious disease expert at UCSF, has stated the B.1.1.7 UK variant has been found in 22 states so far, including 72 cases in California, according to the Centers for Disease Control and Prevention.
The variant in South Africa was first detected in Nelson Mandela Bay in samples dating back to the beginning of October 2020. South Africa showed a sharp rise in the number of infected during November 2020, and reported 501Y.V2 to the World Health Organization on 18 Dec 2020. More than 1.3 million people have been infected with the virus in South Africa, highest of any African nation, more than 37,000 South Africans have died from COVID-19. Most new infections are caused by the 501Y.V2 variant.
Mutations have significantly changed the South African virus’ spike protein; the spike protein has now rotated about twenty degrees and can therefore get more deeply into the binding site on cells; thus, the virus can bind better to human cells, enabling it to become a more efficient virus for transmission. The South Africa variant is about 50% more contagious than the original strain. The Western Cape region took 107 days to reach 100,000 cases in the first wave compared to 54 days in the second wave, when the variant appeared. The South African variant has spread to 14 countries. The director of the Centers for Disease Control and Prevention said, 29 Jan 2021, that the South African Covid-19 variant, which was just detected in two people in South Carolina, had already reached the point of community spread in the U.S. On 9 Jan 2021, Japan notified WHO of a new SARS-CoV-2 variant B.1.1.28 detected in 4 travelers from Brazil. This variant has 12 mutations to the spike protein, including 3 mutations in common with 501Y.V2, ie, K417N/T, E484K and N501Y, which potentially can change transmissibility and host immune responses. Brazil has also reported emergence of a similar variant, with E484K mutation, which evolved independently of the variant from the travelers.
By mid January 2021, Dr. Charles Chiu, director of the UCSF-Abbott Viral Diagnostics and Discovery Center, from sequencing results from his lab at UCSF, found a rare variant, that Chiu had only seen in a handful of samples, suddenly jump up to 25% in his samples. Chiu’s team was the first to report the new variant, now called L452R, but within days, diagnosticians at Cedars-Sinai reported the same variant was now making up more than a third of cases in Los Angeles.
NowDelta (B.1.617.2) variant is currently the most prevalent variant in the United States. New data indicate that the Delta variant spreads almost twice as fast as the original SARS-CoV-2 virus.
These variants suggest specific antiviral measures may be sidestepped by their changes if the measures are targeted too specifically to an antigen. I stated this in an earlier post about monoclonal antibody driving escape mutations by selection pressure. This has been borne out by recent clinical studies. Treatment with bamlanivimab and etesevimab, monoclonal anti-spike antibodies to different epitope targets, of nonhospitalized patients with mild to moderate COVID-19 illness, compared with placebo, showed statistically significant decrease in SARS-CoV-2 viral load at day 11; however, no significant reduction in viral load was seen with bamlanivimab monotherapy. The South African strain has also demonstrated escape from such treatment. It has been observed to completely escape from three monoclonal antibodies, reported by scientists from three South African universities, with the National Institute for Communicable Diseases (NICD), in a paper published on the bioRxiv website (https://bit.ly/2Y0lHEt). In addition, 501Y.V2 showed substantial or complete escape from neutralizing antibodies from COVID-19 convalescent plasma. They concluded reinfection could occur, and the differences in the variant may lead to reduced efficacy of current spike-based vaccines (New COVID-19 Variant Defeats Plasma Treatment, MABs, May Reduce Vaccine Efficacy – Medscape – Jan 20, 2021). Such dire predictions, have led individuals and physicians to pursue broad-spectrum treatments which make such variations irrelevant.
Didier Raoult’s tarnished claim hydroxychloroquine and azithromycin were effective against COVID-19 has not completely died because of this need for a generalized treatment, even in the scientific community. In a recent ACS paper, the investigators used hydroxychloroquine (HCQ) as a reference template to screen for structural similarity against a library of approximately 4000 approved drugs. The top-ranked drugs, based on structural similarity to HCQ, selected for in vitro antiviral assessment, were zuclopenthixol and nebivolol, which blocked SARS-CoV-2 in vitro infection with EC50 values in the low micromolar range. The anti-SARS-CoV-2 potential of ambroxol, amodiaquine, and its active metabolite (N-monodesethyl amodiaquine) were discussed. They concluded both the pKa (acidity) and the HCQ aromatic core play a role in antiviral activity. These are such broad mechanisms that such studies are academic and may have too many in vivo variable interactions to be clinically relevant (Giovanni Bocci et al. ACS Pharmacol. Transl. Sci. 2020, 3, 6, 1278–1292; publication date: October 14, 2020, https://doi.org/10.1021/acsptsci.0c00131). Unfortunately, another anti-parasitic drug, Ivermectin, has been revisited as a general antiviral after 50 years of study that have not translated into such clinical use https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7251046/pdf/210_2020_Article_1902.pdf and https://www.nature.com/articles/s41429-020-0336-z.pdf. Among the many mechanisms of action of Ivermectin, the most relevant to antiviral activity is as an inhibitor of nuclear transport mediated by the importin α/β1 heterodimer, responsible for the translocation of various viral species proteins. Unfortunately, most of the viruses it is supposed to effect are not inhibited in replication or infection, or at least consistently. For HIV type 1, a study showed that Ivermectin failed to control the nuclear accumulation of telomer repeat factor-1 (GFP-TRF) which can only be transferred by IMPβ1 to the cell nucleus disputing the proposed mechanism. Researchers concluded that Ivermectin is not a specific inhibitor for IN-IMP α/β interaction, but it appears to be a specific inhibitor of cargos that are dependent on the heterodimer, making its predicted antiviral activity in a host even more suspicious. Law of diminishing returns seems to come into play with Ivermectin treatment. Virus out runs capacity. In pigs with circovirus 2, in the first 24 hrs, Ivermectin reduced viral load by 41% and 28.2%, However, in 48 hrs, it reduced viral load 28.8% and 15.7%, at the same treatment concentrations. Evidently, it decreases in drug efficacy at later time points of infection. In a recent study among adults with mild COVID-19, a 5-day course of ivermectin, compared with placebo, did not significantly improve the time to resolution of symptoms. The findings did not support the use of ivermectin for treatment of mild COVID-19 https://jamanetwork.com/journals/jama/articlepdf/2777389/jama_lpezmedina_2021_oi_210022_1614808764.76432.pdf. In spite of all its years of use in Veterinary Medicine, to prevent heartworms in dogs and other worms in livestock, I have never heard of a veterinarian using it to treat viral infections. Also, I don’t see Ivermectin listed in the Overview of Antiviral Agents, Pharmacology, in the Merck Veterinary Manual. For Ivermectin to be effective against SARS-CoV-2, in cell culture, the concentrations had to be in the microgram per ml range, blood levels of Ivermectin are at safe therapeutic doses in the 20–80 ng/ml range.
The National Institutes of Health (NIH), under pressure from clinicians, has dropped its recommendation against the inexpensive antiparasitic drug Ivermectin for treatment of COVID-19, and the agency now states it can’t recommend for or against its use, leaving the decision to physicians and their patients. “Results from adequately powered, well-designed, and well-conducted clinical trials are needed to provide more specific, evidence-based guidance on the role of ivermectin for the treatment of COVID-19,” according to new NIH guidance released recently. Some clinical studies showed no benefits or worsening of disease after its use; however, others reported shorter time to resolution of disease. This may be tied to viral load or just an unreliable, unpredictable response.
Some have already failed clinical trials (such as hydroxychloroquine) and some seem counterintuitive (like the immunosuppressant cyclosporine) so caution must be taken in extrapolating these results and they only be considered for suggesting possible clinical testing candidates. They found nine drugs with antiviral activity in lung epithelial cells: 7 of the drugs have been used in humans, 3 FDA approved in the United States (cyclosporine, dacomitinib, and salinomycin), and ebastine (an anti-histamine) approved outside the United States (https://www.cell.com/action/showPdf?pii=S2211-1247%2821%2900273-4). Some of the immunosuppressive and ant-histamine anti-SARS-CoV-2 activities may be explained by the linkage of the host response to the virus to the peculiar anti-parasite, anti-tumor immunity and its adverse effects in COVID.
Other non-immune-mediated drugs are being considered. The government is paying Merck & Co about 356 million USD to fast-track production of one of its potential treatments under Operation Warp Speed. The funding will allow the company to deliver up to 100,000 doses by 30 June 2021, if successful and FDA clears the treatment for emergency use. It is called MK-7110, designed to minimize damaging effects of an overactive immune response to COVID-19. Another promising drug is plitidepsin (aplidin), 27.5 times more potent than remdesivir in cell culture. The mechanism of action against SARS-CoV-2 is through inhibiting eEF1A, a key cellular protein in proliferation and growth (the eukaryotic elongation factor 1 α, eEF1A). During protein translation, eEF1A recruits aminoacyl t-RNA to the ribosome and translocates the growing polypeptide from the ribosomal A site to the P site. Therefore, the drug inhibits viral protein production and, subsequently, viral replication. It’s potential toxicity, because of this non-specificity, is on protein synthesis, growth and healing. The viral production was inhibited at 8-12 hours but was not significant after 24 hours of infection. Therefore, it must be used early in infection based on these in vitro and animal studies https://science.sciencemag.org/content/sci/early/2021/01/22/science.abf4058.full.pdf. Recently modeling efforts and in vitro cell culture studies have examined repurposing other FDA approved drugs as antivirals to treat COVID. These include the old anti-tapeworm drug niclosamide. It has shown broad efficacy against viruses including SARS-CoV-2. This salicylanilide’s antiviral activity is based on its ability to prevent acidification of endocytotic compartments, blocking membrane fusion and infection of the host cell. Early viral studies showed that the efficacy of salicylanilides was derived from the anilide ring, the important role of the N− H group in shuttling protons into the endosome. Niclosamide’s reduction of infection in cells without interacting directly with any viral components presents the possibility of anti-COVID-19 therapeutics with broad activity against current and future variants of the virus, but also may dilute out its effectiveness as seen with antihelmintics like ivermectin and increase the possibility of side effects (Steven Blake et al., Salicylanilides Reduce SARS-CoV‐2 Replication and Suppress Induction of Inflammatory Cytokines in a Rodent Model, https://doi.org/10.1021/acsinfecdis.1c00253 A, ACS Infect. Dis.).
How do we reconcile broad-spectrum, non-specific treatments to counter natural selection of viruses resistant to specific antibody or cellular immunity against requirements to avoid off-target and diluted-out effects of non-specific treatments ? First, the current vaccines may induce broader coverage immunity than illustrated by monoclonal antibody or convalescent plasma responses to infection. Even the difference between male and female immune responses, females having more effective T cell cellular immune responses than males’ B cell dominated antibody response, indicates broader immune coverage from the same SARS-CoV-2 antigens https://science.sciencemag.org/content/sci/371/6527/347.full.pdf. The Th17 response to COVID-19 also indicates a more generalized polyclonal immune response. So don’t write off the current vaccines yet. Second, I have alluded to, in earlier posts, that aptamers which can be selected synthetically to many targets on the virus and be changed rapidly, can also link these anti-ligands to specific pre-existing antibody or immune cells to rapidly mobilize the immune system against the virus and even convert the pathogenic virus into an autogenous endogenous vaccine after directly neutralizing it. The original route of administration was by inhalation to enable self-application of the treatment/prevention. However, these approaches are yet to get out of the basic research laboratory.
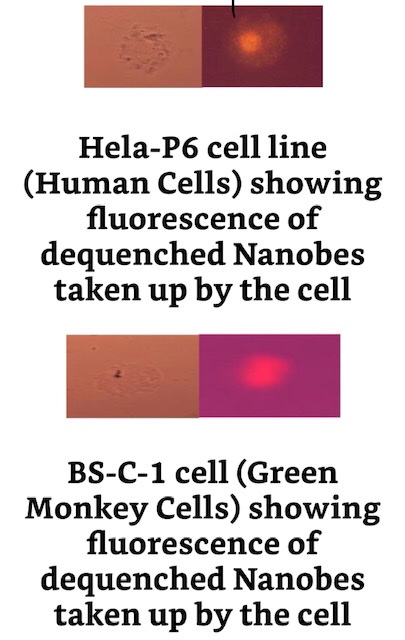
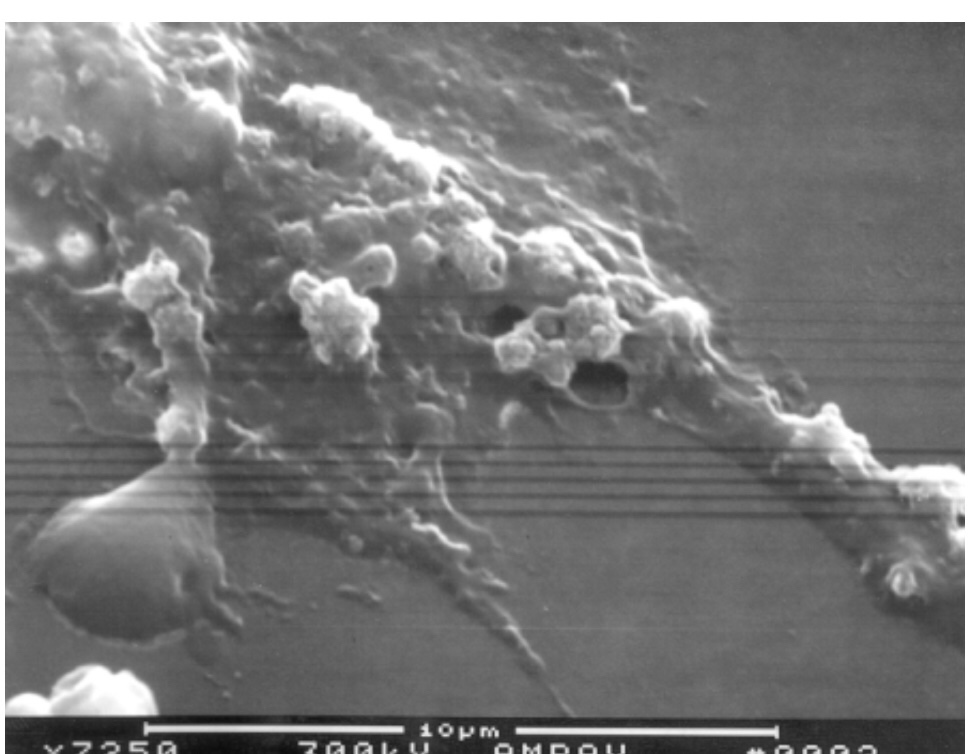
Demonstration of the concept of re-directing the immune system is illustrated by data in this patent showing that previous inoculation with human serum (stand-in for a vaccination) helps decrease lethality of inhaled anthrax spores through an alpha-gal carbohydrate component of aptamers, against which antibody in the human serum is naturally immune, and a linked component of the same aptamers selected in vitro to bind to the protective antigen (PA) of the anthrax toxin. The mouse antibody against the human antibody against the alpha-gal on the aptamers is directed to mediate immune inactivation of the whole toxin, reducing the lethality of anthrax from the spores. Even more remarkable is that the aptamer was delivered by inhalation as well.Method of making aptamers against any infectious disease agent rapidly on demandBetter untapped way: Synthetic Nanobes can carry the nitrate reductase gene, an alpha virus (VEEV) RNA dependent RNA polymerase gene, and pathogen-specific aptamer sequences as well as aptamer immune cell and existing antibody linker aptamer sequences which re-direct existing immunity immediately toward new antigens such as those developed in a new variant pathogen mutant—tit for tat anti-virus selected mutations. These Nanobes can become adapters for old vaccine to new variants of pathogenic viruses and the Nanobes become self-replicating RNA forms that can move from cell to cell in the host, but still have a fail-safe self-destruct mechanism (non-ionizing electromagnetic radiation absorption to destruction) and regulating nutrients required for replication — nitrate and 3-amino-L-tyrosine. This should be seen as a tool for new treatments and rejuvenation of the effectiveness of old vaccines to address new variants, not a panacea but an enduring platform.Showing carbon nanotubes can carry genes into cellsAnother method of tracing the movement of gene-bearing Nanobes into living cells: fluorescence
HeLa-NR1cells producing and extruding biosynthetic clusters of polymer nanoparticles (white) capable of carrying cell-synthesized RNA
The cycle of totally synthetic Nanobes to totally self-replicating biosynthetic Nanobes. SNA= small synthetic nucleic acid; SWCNT= single walled carbon nanotube; NP= nanoparticle; DALM= diazoluminomelanin; the photomicrograph is of live cells in culture expressing Green Fluorescent Protein (GFP) after transfection with totally synthetic Nanobes carrying the gene.
You are probably sick of me saying this over and over again, but ignoring these facts and principles does not end the pandemic only makes it worse:
My book Pathogenic Ecology points out in detail how we get into such a mess and why we can’t ignore it:
Re-posting this post because of its prophetic content: The viruses, including SARS-CoV-2, continue to evolve by mutation and selection toward being more efficient at infection and transmission within close, tight social groups but falling off quickly when vaccination and moderate barriers, like masks and good ventilation, and social distancing are implemented.
Vaccination does NOT guarantee protection from infection by Delta variant or transient release of virus from asymptomatic vaccinated individuals. Vaccination is NOT for elimination of all possible virus but to reduce infection level below the point of symptoms of disease in immunized people (varies from person to person somewhat, but is more likely to be overcome with higher circulating viral loads). It is the circulating of more infectious particles over and over so there can be accumulation and increased probability of developing more mutants, therefore, variants, that is problematic. Also, we have no way of screening or asking the vaccine status, health status or contact status of those entering a high density environment. Therefore, I recommend wearing a mask as well, regardless of vaccine status, and for others with any immunocompromizing condition or respiratory illness, especially with fever in the last 10 days, not to attend such event locations. The more people present, knowingly or unknowingly infected, the more virus circulating and the more likely to overcome vaccination,
This post is a summary in lay, non-technical terms, of what we know about COVID and the virus that causes it, amongst its kind. I will couch this description in military terms and as if the virus enemy is a sentient being because of my military background. The analogy is only for illustration and not proof of what I say. Our story, in late 2019, early 2020, began with a foreboding of the consequences of our happy hurried ignorance of larger life and the cost of practicing ignorance of it when confronting it head on : “Violent Delights, Violent Ends: Fire and Powder, Kiss and Consume”, “I fear too early, for my mind misgives some consequence yet hanging in the stars shall bitterly begin this fearful date with this night’s revels, and expire the term of ….. life ….. by some vile forfeit of untimely death….” William Shakespeare, Romeo and Juliet, Act 1, Scene 4”. There is an elegance in design in what we have faced and experienced when we look past the undeniable tragedy, which should never be forgotten as a great battle is remembered, which we must admit we have lost to learn from it, in our ongoing war with microbes, and the missteps that led to it. We started with underestimating our enemy. After all, most physicians’ experience with coronaviruses is the cold-causing, self-limiting, take-an-aspirin-and-call-me-in-morning ones successfully treated by benign neglect. Even the serious ones like SARS 1 (Severe Acute Respiratory Syndrome Virus, from civet cats, originally from bats), which appeared in 2003 and disappeared in 6 months, and MERS (Middle East Respiratory Syndrome Virus, from camels, originally from bats), which has only spread slowly in the Middle East and Northern Africa, were largely ignored as harbingers of something worse to come. In our arrogance and ignorance, we thought they disappeared or were restricted because of expert human interference; we ignored the warning of “some consequence yet hanging in the stars” of something much worse. Not only physicians fed this false security (besides the inevitable politicians at the top), but also veterinarians, who thought coronaviruses were under control. We have seen coronaviruses pervasively in dogs, cats, cattle and birds, but largely of the young, from self-limiting, and diminishing as agents necessitating prevention by vaccination, especially in dogs, to vaccination effective, but not fully optimal control (focusing on the pregnant females or newborns to produce immunity even if transient or against disease but not infection), in preventing large economic losses in intensive bovine, porcine, and poultry production. This requirement makes their use routine and necessary in agriculture, especially in preventing respiratory disease losses in poultry, and losses in calves and pigs from hemorrhagic diarrhea and shipping fever complex in finishing out beef cattle. However, in birds, live attenuated vaccine viruses have been detected circulating in wild bird populations, leading to potential recombination with or mutation to pathogenic strains. Only in the virus that causes Feline Infectious Peritonitis (FIP), which is usually 100% fatal in young cats showing signs but showing few signs, if any, and self-limiting when the kittens are infected with a less lethal strain of the virus (most often), was there evidence of something persistent and on occasion much more lethal. Presently, veterinarians are attempting to treat FIP with the same antiviral drugs as COVID over very protracted times, prolonging life but struggling to get cures. Not even this foreshadowing of the enemy becoming capable of new more insidious and dangerous strategies was heeded. One health appeared to learn nothing from these experiences until the stealthy tragedy of COVID was upon the world. The FIP lesson of a virus that is highly infectious and widespread in close collections of cats, which could largely be ignored and not even worth vaccination, could on occasion, when symptomatic, kill with such lethality, was attributed solely to a rare emergence of a selected highly lethal strain. However, although it appears again and again, it never seems to get an epizootic foot hold, killing only a few or one cat in a close knit group. Where does it go? Why does it keep coming back in such a limited way? No very satisfactory answers. But it surely appears to have an uncanny, but not as well developed, resemblance to the COVID modus operandi—myth of a largely non-symptomatic disease, low overall mortality, until in reality it becomes severely symptomatic and then lethality jumps sky high. These characteristics feed the denial and false claims of inflated lethality for COVID. Unfortunately, this feeds more careless spread of the virus. Could this be its evolutionary “intent” ?
Since it’s discovery in 2006, ferret systemic coronavirosis has been an emerging fatal disease of ferrets caused by ferret systemic coronavirus (FRSCV) which shares clinical-pathological characteristics with the dry form of feline infectious peritonitis (FIP) in cats. Because of the vulnerability of mustelidae (a family of carnivorous mammals, including weasels, badgers, otters, ferrets, martens, minks and wolverines, among others, a diverse group which forms the largest family in the order Carnivora, suborder Caniformia, comprising about 56–60 species across eight subfamilies) to both FIP (ferret coronavirus) and SARS-CoV-2, these animals potentially link the pathology of FIP to SARS-CoV-2, at least deserving further study.
The major strategy change of the COVID virus from the others, especially animal ones (although all coronaviruses are zoonotic, the cold ones appearing to have originated in rodents, cattle and some unknown animal eons ago), has been to sparing the young of disease, although still being asymptomatic in most age groups, except the old and infirm. Its infectivity in cats, minks and ferrets, says SARS-CoV-2 (originating in bats) is still very much an animal virus. It still holds in common with all coronaviruses the goal of not burning through a host population so as to prevent herd immunity and always to have susceptible individuals in that population to maintain them indefinitely. Even in the most densely populated and numerous mammals in nature, perhaps only second to humans, bats, coronaviruses only infect about 10% of a given group at a time. Pathogenicity and lethality tend to be held in check except in individuals in a population that do not contribute to maintenance of the virus in the population, like the elderly and infirm who do not reproduce individuals vulnerable to infection and transmission. Why is COVID different from animals in these respects of populations? The answer may lie in that animal viruses establish carriers by preferring gastrointestinal infections that are not easily cleared and chronically shed transmissible virus. In other viruses, like influenza, especially in migratory birds and water fowl, it is predominantly a GI rather than respiratory virus, which most effectively maintains the birds as a reservoir rather than incapacitating or killing the birds, which would limit their ability to spread the viruses. The COVID virus has chosen a more unorthodox method to assure maintenance and transmission in the human population, although with time I believe we will find more and more asymptomatic GI shedders (by monitoring sewage which has begun) https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.25825 and https://www.medrxiv.org/content/10.1101/2021.01.08.21249379v1. It has chosen to enhance anti-parasite immunity like that used by the hosts to control parasitic worm, pathogenic protozoan and fungal infestations and infections. This response often controls the number of parasites to a tolerable, but not immediately lethal, level and prevents further infestation (a process called premunition), but does not totally eliminate the parasite. In children, this form of innate non-specific immunity often rapidly clears an infection without inducing long term immunity. Therefore, they are allowed to survive, grow and reproduce more naive vulnerable individuals after spreading the virus in the population. They are also vulnerable to re-infection as they grow older. Adults can mount this type of immunity but then develop specific adaptive long term immunity, but unfortunately also “memory” of the initial innate response with a vengeance. If this “remembered” non-specific response becomes overt or is activated, as it is highly vulnerable to do, by non-viral stimuli, it can lead to autoimmunity and pro-inflammatory nonspecific disease, which has been observed in “long haulers”. The fatal severe COVID is a continuum of the infection from inapparent widespread tissue infection to a late activation of this parasite immunity to the extreme, death, without a break. This type of incomplete immunity is beneficial for resisting parasites and in tumor immunology because it is highly effective locally, but suppressed systemically to avoid collateral damage to normal self tissues.
I have observed an artificial reproduction, perhaps enhancement, or at least a mimic, of this type of reactive oxygen species innate immunity early in my research career. I described it in my first book . “Even though weaker, nonspecific cytotoxicity was expected with glucose oxidase and horseradish peroxidase, they were used. Very malignant Novikoff hepatocarcinoma (including metastases) in rats, spontaneous mammary adenocarcinomas in rats, L1210 leukemia in mice, B16 melanomas in mice, and carcinogen-induced squamous cell carcinomas in hamster cheek pouches all responded to regional or local injections of the cross-linked enzymes in saline and glucose solution. The Novikoff hepatocarcinoma responses were 50 to 100% cures in animals treated. Lactoperoxidase could be substituted for horseradish peroxidase, and similar results were obtained. However, galactose oxidase substitution or the absence of either the glucose oxidase or the respective peroxidase in the preparation failed to bring about tumor regression. L1210 leukemia in outbred white mice showed 50% cures. Treatment of B16 melanoma prolonged life from 23 days postinoculation of controls to 37 days with treatment. However, no simple dose-response curve was demonstrated..Also, smaller squamous cell carcinoma tumors responded better (some with cures) than did larger cheek pouch tumors, which did not respond at all..No direct injury to normal tissue was observed in histopathological sections of treated animals. However, some animals with heavy tumor loads (P388 lymphoma, L1210 leukemia, some with Novikoff hepatocarcinoma) died more quickly when treated than did untreated controls due to an apparent “necrotic crisis” from dying tumor tissue.”— Type-B Cytochromes: Sensors and Switches by J.L. Kiel. https://a.co/aJEAVsl. I was acutely aware of the relationship between oxidase/peroxidase innate non-specific immunity and resistance to parasites and cancer because I entered Texas Tech University Health Science Center, School of Medicine, Graduate School, in the Departments of Biochemistry and Microbiology, as one of their first PhD students, in the summer of 1977 at Lubbock, Texas, with the intent to study this anti-parasitic mechanism. My dissertation research was on the cytotoxic mechanisms of peroxidases, a principle antimicrobial and anti-parasitic enzyme in granulocytes and macrophages of animals and humans. I wanted to study the effects of eosinophilic peroxidase on blood flukes (an animal counterpart of Schistosoma called Heterobilharzia americana) but my graduate committee and the safety officer would not approve of my keeping my infected snails in an aquarium in the laboratory. Therefore, I turned to peroxidase killing of cancer cells.
This highly localized approach is necessary because parasites and cancers disguise themselves as normal host tissue and this type of immunity must attack them without confusing them with normal tissue, which could be fatal or at least highly damaging to normal tissues and organs. It is a very delicate balance that could go either way. Therefore, any treatments or vaccines must direct a response that limits early replication of the virus and do not trigger an overt systemic parasite immune response. Hopefully, the current vaccines and treatments currently being evaluated will do this.
As a final personal note, I dealt, in my professional lifetime, with trying to address these mechanisms in other infectious zoonotic diseases and where infectious agents come from, go to between outbreaks, and how to stop them from re-emerging and spreading. By my measure, what has happened with COVID-19 would have been a total failure if it had been in my purview of investigative and applied functions and responsibilities. I spent the first third of my career investigating the non-specific responses to chemical, biological, and radiation insults, especially non-ionizing electromagnetic radiation, microwaves and radiowaves, and the second two thirds investigating means to detect hidden infectious agents and to stop re-emergence of infectious agents from between outbreaks. You may question my authority and knowledge in this area and assume I should have some honored and respected position in academia or industry after my retirement from serving the military and nation. I do not. It appears the arts and sciences of attribution and Counterproliferation of biological agents, natural or nefarious, are so specialized that there is no venerable honored academic or industrial positions or no longer governmental positions that meet with my qualifications. Since my retirement in 2011 and being turned down many times for academic positions, I have only been called on by the federal government when emergency situations required my services and was summarily dismissed when the crisis passed. However, when the crisis occurs, as with COVID, is when my talents are least but albeit still critically effective if heeded. I thought that even at 71, I might be valuable in sharing my experience, knowledge and insights with those who need to follow me in these pursuits, which I did in the military, but am not allowed to do now except by my books, past publications and currently this blog. I will continue as long as one person reads this blog and am able to continue.
You are probably sick of me saying this over and over again, but ignoring these facts and principles does not end the pandemic only makes it worse:
My book Pathogenic Ecology points out in detail how we get into such a mess and why we can’t ignore it:
Re-posting this post because of its prophetic content: The viruses, including SARS-CoV-2, continue to evolve by mutation and selection toward being more efficient at infection and transmission within close, tight social groups but falling off quickly when vaccination and moderate barriers, like masks and good ventilation, and social distancing are implemented.
Vaccination does NOT guarantee protection from infection by Delta variant or transient release of virus from asymptomatic vaccinated individuals. Vaccination is NOT for elimination of all possible virus but to reduce infection level below the point of symptoms of disease in immunized people (varies from person to person somewhat, but is more likely to be overcome with higher circulating viral loads). It is the circulating of more infectious particles over and over so there can be accumulation and increased probability of developing more mutants, therefore, variants, that is problematic. Also, we have no way of screening or asking the vaccine status, health status or contact status of those entering a high density environment. Therefore, I recommend wearing a mask as well, regardless of vaccine status, and for others with any immunocompromizing condition or respiratory illness, especially with fever in the last 10 days, not to attend such event locations. The more people present, knowingly or unknowingly infected, the more virus circulating and the more likely to overcome vaccination,
This post is a summary in lay, non-technical terms, of what we know about COVID and the virus that causes it, amongst its kind. I will couch this description in military terms and as if the virus enemy is a sentient being because of my military background. The analogy is only for illustration and not proof of what I say. Our story, in late 2019, early 2020, began with a foreboding of the consequences of our happy hurried ignorance of larger life and the cost of practicing ignorance of it when confronting it head on : “Violent Delights, Violent Ends: Fire and Powder, Kiss and Consume”, “I fear too early, for my mind misgives some consequence yet hanging in the stars shall bitterly begin this fearful date with this night’s revels, and expire the term of ….. life ….. by some vile forfeit of untimely death….” William Shakespeare, Romeo and Juliet, Act 1, Scene 4”. There is an elegance in design in what we have faced and experienced when we look past the undeniable tragedy, which should never be forgotten as a great battle is remembered, which we must admit we have lost to learn from it, in our ongoing war with microbes, and the missteps that led to it. We started with underestimating our enemy. After all, most physicians’ experience with coronaviruses is the cold-causing, self-limiting, take-an-aspirin-and-call-me-in-morning ones successfully treated by benign neglect. Even the serious ones like SARS 1 (Severe Acute Respiratory Syndrome Virus, from civet cats, originally from bats), which appeared in 2003 and disappeared in 6 months, and MERS (Middle East Respiratory Syndrome Virus, from camels, originally from bats), which has only spread slowly in the Middle East and Northern Africa, were largely ignored as harbingers of something worse to come. In our arrogance and ignorance, we thought they disappeared or were restricted because of expert human interference; we ignored the warning of “some consequence yet hanging in the stars” of something much worse. Not only physicians fed this false security (besides the inevitable politicians at the top), but also veterinarians, who thought coronaviruses were under control. We have seen coronaviruses pervasively in dogs, cats, cattle and birds, but largely of the young, from self-limiting, and diminishing as agents necessitating prevention by vaccination, especially in dogs, to vaccination effective, but not fully optimal control (focusing on the pregnant females or newborns to produce immunity even if transient or against disease but not infection), in preventing large economic losses in intensive bovine, porcine, and poultry production. This requirement makes their use routine and necessary in agriculture, especially in preventing respiratory disease losses in poultry, and losses in calves and pigs from hemorrhagic diarrhea and shipping fever complex in finishing out beef cattle. However, in birds, live attenuated vaccine viruses have been detected circulating in wild bird populations, leading to potential recombination with or mutation to pathogenic strains. Only in the virus that causes Feline Infectious Peritonitis (FIP), which is usually 100% fatal in young cats showing signs but showing few signs, if any, and self-limiting when the kittens are infected with a less lethal strain of the virus (most often), was there evidence of something persistent and on occasion much more lethal. Presently, veterinarians are attempting to treat FIP with the same antiviral drugs as COVID over very protracted times, prolonging life but struggling to get cures. Not even this foreshadowing of the enemy becoming capable of new more insidious and dangerous strategies was heeded. One health appeared to learn nothing from these experiences until the stealthy tragedy of COVID was upon the world. The FIP lesson of a virus that is highly infectious and widespread in close collections of cats, which could largely be ignored and not even worth vaccination, could on occasion, when symptomatic, kill with such lethality, was attributed solely to a rare emergence of a selected highly lethal strain. However, although it appears again and again, it never seems to get an epizootic foot hold, killing only a few or one cat in a close knit group. Where does it go? Why does it keep coming back in such a limited way? No very satisfactory answers. But it surely appears to have an uncanny, but not as well developed, resemblance to the COVID modus operandi—myth of a largely non-symptomatic disease, low overall mortality, until in reality it becomes severely symptomatic and then lethality jumps sky high. These characteristics feed the denial and false claims of inflated lethality for COVID. Unfortunately, this feeds more careless spread of the virus. Could this be its evolutionary “intent” ?
Since it’s discovery in 2006, ferret systemic coronavirosis has been an emerging fatal disease of ferrets caused by ferret systemic coronavirus (FRSCV) which shares clinical-pathological characteristics with the dry form of feline infectious peritonitis (FIP) in cats. Because of the vulnerability of mustelidae (a family of carnivorous mammals, including weasels, badgers, otters, ferrets, martens, minks and wolverines, among others, a diverse group which forms the largest family in the order Carnivora, suborder Caniformia, comprising about 56–60 species across eight subfamilies) to both FIP (ferret coronavirus) and SARS-CoV-2, these animals potentially link the pathology of FIP to SARS-CoV-2, at least deserving further study.
The major strategy change of the COVID virus from the others, especially animal ones (although all coronaviruses are zoonotic, the cold ones appearing to have originated in rodents, cattle and some unknown animal eons ago), has been to sparing the young of disease, although still being asymptomatic in most age groups, except the old and infirm. Its infectivity in cats, minks and ferrets, says SARS-CoV-2 (originating in bats) is still very much an animal virus. It still holds in common with all coronaviruses the goal of not burning through a host population so as to prevent herd immunity and always to have susceptible individuals in that population to maintain them indefinitely. Even in the most densely populated and numerous mammals in nature, perhaps only second to humans, bats, coronaviruses only infect about 10% of a given group at a time. Pathogenicity and lethality tend to be held in check except in individuals in a population that do not contribute to maintenance of the virus in the population, like the elderly and infirm who do not reproduce individuals vulnerable to infection and transmission. Why is COVID different from animals in these respects of populations? The answer may lie in that animal viruses establish carriers by preferring gastrointestinal infections that are not easily cleared and chronically shed transmissible virus. In other viruses, like influenza, especially in migratory birds and water fowl, it is predominantly a GI rather than respiratory virus, which most effectively maintains the birds as a reservoir rather than incapacitating or killing the birds, which would limit their ability to spread the viruses. The COVID virus has chosen a more unorthodox method to assure maintenance and transmission in the human population, although with time I believe we will find more and more asymptomatic GI shedders (by monitoring sewage which has begun) https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.25825 and https://www.medrxiv.org/content/10.1101/2021.01.08.21249379v1. It has chosen to enhance anti-parasite immunity like that used by the hosts to control parasitic worm, pathogenic protozoan and fungal infestations and infections. This response often controls the number of parasites to a tolerable, but not immediately lethal, level and prevents further infestation (a process called premunition), but does not totally eliminate the parasite. In children, this form of innate non-specific immunity often rapidly clears an infection without inducing long term immunity. Therefore, they are allowed to survive, grow and reproduce more naive vulnerable individuals after spreading the virus in the population. They are also vulnerable to re-infection as they grow older. Adults can mount this type of immunity but then develop specific adaptive long term immunity, but unfortunately also “memory” of the initial innate response with a vengeance. If this “remembered” non-specific response becomes overt or is activated, as it is highly vulnerable to do, by non-viral stimuli, it can lead to autoimmunity and pro-inflammatory nonspecific disease, which has been observed in “long haulers”. The fatal severe COVID is a continuum of the infection from inapparent widespread tissue infection to a late activation of this parasite immunity to the extreme, death, without a break. This type of incomplete immunity is beneficial for resisting parasites and in tumor immunology because it is highly effective locally, but suppressed systemically to avoid collateral damage to normal self tissues.
I have observed an artificial reproduction, perhaps enhancement, or at least a mimic, of this type of reactive oxygen species innate immunity early in my research career. I described it in my first book . “Even though weaker, nonspecific cytotoxicity was expected with glucose oxidase and horseradish peroxidase, they were used. Very malignant Novikoff hepatocarcinoma (including metastases) in rats, spontaneous mammary adenocarcinomas in rats, L1210 leukemia in mice, B16 melanomas in mice, and carcinogen-induced squamous cell carcinomas in hamster cheek pouches all responded to regional or local injections of the cross-linked enzymes in saline and glucose solution. The Novikoff hepatocarcinoma responses were 50 to 100% cures in animals treated. Lactoperoxidase could be substituted for horseradish peroxidase, and similar results were obtained. However, galactose oxidase substitution or the absence of either the glucose oxidase or the respective peroxidase in the preparation failed to bring about tumor regression. L1210 leukemia in outbred white mice showed 50% cures. Treatment of B16 melanoma prolonged life from 23 days postinoculation of controls to 37 days with treatment. However, no simple dose-response curve was demonstrated..Also, smaller squamous cell carcinoma tumors responded better (some with cures) than did larger cheek pouch tumors, which did not respond at all..No direct injury to normal tissue was observed in histopathological sections of treated animals. However, some animals with heavy tumor loads (P388 lymphoma, L1210 leukemia, some with Novikoff hepatocarcinoma) died more quickly when treated than did untreated controls due to an apparent “necrotic crisis” from dying tumor tissue.”— Type-B Cytochromes: Sensors and Switches by J.L. Kiel. https://a.co/aJEAVsl. I was acutely aware of the relationship between oxidase/peroxidase innate non-specific immunity and resistance to parasites and cancer because I entered Texas Tech University Health Science Center, School of Medicine, Graduate School, in the Departments of Biochemistry and Microbiology, as one of their first PhD students, in the summer of 1977 at Lubbock, Texas, with the intent to study this anti-parasitic mechanism. My dissertation research was on the cytotoxic mechanisms of peroxidases, a principle antimicrobial and anti-parasitic enzyme in granulocytes and macrophages of animals and humans. I wanted to study the effects of eosinophilic peroxidase on blood flukes (an animal counterpart of Schistosoma called Heterobilharzia americana) but my graduate committee and the safety officer would not approve of my keeping my infected snails in an aquarium in the laboratory. Therefore, I turned to peroxidase killing of cancer cells.
This highly localized approach is necessary because parasites and cancers disguise themselves as normal host tissue and this type of immunity must attack them without confusing them with normal tissue, which could be fatal or at least highly damaging to normal tissues and organs. It is a very delicate balance that could go either way. Therefore, any treatments or vaccines must direct a response that limits early replication of the virus and do not trigger an overt systemic parasite immune response. Hopefully, the current vaccines and treatments currently being evaluated will do this.
As a final personal note, I dealt, in my professional lifetime, with trying to address these mechanisms in other infectious zoonotic diseases and where infectious agents come from, go to between outbreaks, and how to stop them from re-emerging and spreading. By my measure, what has happened with COVID-19 would have been a total failure if it had been in my purview of investigative and applied functions and responsibilities. I spent the first third of my career investigating the non-specific responses to chemical, biological, and radiation insults, especially non-ionizing electromagnetic radiation, microwaves and radiowaves, and the second two thirds investigating means to detect hidden infectious agents and to stop re-emergence of infectious agents from between outbreaks. You may question my authority and knowledge in this area and assume I should have some honored and respected position in academia or industry after my retirement from serving the military and nation. I do not. It appears the arts and sciences of attribution and Counterproliferation of biological agents, natural or nefarious, are so specialized that there is no venerable honored academic or industrial positions or no longer governmental positions that meet with my qualifications. Since my retirement in 2011 and being turned down many times for academic positions, I have only been called on by the federal government when emergency situations required my services and was summarily dismissed when the crisis passed. However, when the crisis occurs, as with COVID, is when my talents are least but albeit still critically effective if heeded. I thought that even at 71, I might be valuable in sharing my experience, knowledge and insights with those who need to follow me in these pursuits, which I did in the military, but am not allowed to do now except by my books, past publications and currently this blog. I will continue as long as one person reads this blog and am able to continue.
My book Pathogenic Ecology points out in detail how we get into such a mess and why we can’t ignore it:
Re-posting this post because of its prophetic content: The viruses, including SARS-CoV-2, continue to evolve by mutation and selection toward being more efficient at infection and transmission within close, tight social groups but falling off quickly when vaccination and moderate barriers, like masks and good ventilation, and social distancing are implemented.
Vaccination does NOT guarantee protection from infection by Delta variant or transient release of virus from asymptomatic vaccinated individuals. Vaccination is NOT for elimination of all possible virus but to reduce infection level below the point of symptoms of disease in immunized people (varies from person to person somewhat, but is more likely to be overcome with higher circulating viral loads). It is the circulating of more infectious particles over and over so there can be accumulation and increased probability of developing more mutants, therefore, variants, that is problematic. Also, we have no way of screening or asking the vaccine status, health status or contact status of those entering a high density environment. Therefore, I recommend wearing a mask as well, regardless of vaccine status, and for others with any immunocompromizing condition or respiratory illness, especially with fever in the last 10 days, not to attend such event locations. The more people present, knowingly or unknowingly infected, the more virus circulating and the more likely to overcome vaccination,
This post is a summary in lay, non-technical terms, of what we know about COVID and the virus that causes it, amongst its kind. I will couch this description in military terms and as if the virus enemy is a sentient being because of my military background. The analogy is only for illustration and not proof of what I say. Our story, in late 2019, early 2020, began with a foreboding of the consequences of our happy hurried ignorance of larger life and the cost of practicing ignorance of it when confronting it head on : “Violent Delights, Violent Ends: Fire and Powder, Kiss and Consume”, “I fear too early, for my mind misgives some consequence yet hanging in the stars shall bitterly begin this fearful date with this night’s revels, and expire the term of ….. life ….. by some vile forfeit of untimely death….” William Shakespeare, Romeo and Juliet, Act 1, Scene 4”. There is an elegance in design in what we have faced and experienced when we look past the undeniable tragedy, which should never be forgotten as a great battle is remembered, which we must admit we have lost to learn from it, in our ongoing war with microbes, and the missteps that led to it. We started with underestimating our enemy. After all, most physicians’ experience with coronaviruses is the cold-causing, self-limiting, take-an-aspirin-and-call-me-in-morning ones successfully treated by benign neglect. Even the serious ones like SARS 1 (Severe Acute Respiratory Syndrome Virus, from civet cats, originally from bats), which appeared in 2003 and disappeared in 6 months, and MERS (Middle East Respiratory Syndrome Virus, from camels, originally from bats), which has only spread slowly in the Middle East and Northern Africa, were largely ignored as harbingers of something worse to come. In our arrogance and ignorance, we thought they disappeared or were restricted because of expert human interference; we ignored the warning of “some consequence yet hanging in the stars” of something much worse. Not only physicians fed this false security (besides the inevitable politicians at the top), but also veterinarians, who thought coronaviruses were under control. We have seen coronaviruses pervasively in dogs, cats, cattle and birds, but largely of the young, from self-limiting, and diminishing as agents necessitating prevention by vaccination, especially in dogs, to vaccination effective, but not fully optimal control (focusing on the pregnant females or newborns to produce immunity even if transient or against disease but not infection), in preventing large economic losses in intensive bovine, porcine, and poultry production. This requirement makes their use routine and necessary in agriculture, especially in preventing respiratory disease losses in poultry, and losses in calves and pigs from hemorrhagic diarrhea and shipping fever complex in finishing out beef cattle. However, in birds, live attenuated vaccine viruses have been detected circulating in wild bird populations, leading to potential recombination with or mutation to pathogenic strains. Only in the virus that causes Feline Infectious Peritonitis (FIP), which is usually 100% fatal in young cats showing signs but showing few signs, if any, and self-limiting when the kittens are infected with a less lethal strain of the virus (most often), was there evidence of something persistent and on occasion much more lethal. Presently, veterinarians are attempting to treat FIP with the same antiviral drugs as COVID over very protracted times, prolonging life but struggling to get cures. Not even this foreshadowing of the enemy becoming capable of new more insidious and dangerous strategies was heeded. One health appeared to learn nothing from these experiences until the stealthy tragedy of COVID was upon the world. The FIP lesson of a virus that is highly infectious and widespread in close collections of cats, which could largely be ignored and not even worth vaccination, could on occasion, when symptomatic, kill with such lethality, was attributed solely to a rare emergence of a selected highly lethal strain. However, although it appears again and again, it never seems to get an epizootic foot hold, killing only a few or one cat in a close knit group. Where does it go? Why does it keep coming back in such a limited way? No very satisfactory answers. But it surely appears to have an uncanny, but not as well developed, resemblance to the COVID modus operandi—myth of a largely non-symptomatic disease, low overall mortality, until in reality it becomes severely symptomatic and then lethality jumps sky high. These characteristics feed the denial and false claims of inflated lethality for COVID. Unfortunately, this feeds more careless spread of the virus. Could this be its evolutionary “intent” ? The major strategy change of the COVID virus from the others, especially animal ones (although all coronaviruses are zoonotic, the cold ones appearing to have originated in rodents, cattle and some unknown animal eons ago), has been to sparing the young of disease, although still being asymptomatic in most age groups, except the old and infirm. Its infectivity in cats, minks and ferrets, says SARS-CoV-2 (originating in bats) is still very much an animal virus. It still holds in common with all coronaviruses the goal of not burning through a host population so as to prevent herd immunity and always to have susceptible individuals in that population to maintain them indefinitely. Even in the most densely populated and numerous mammals in nature, perhaps only second to humans, bats, coronaviruses only infect about 10% of a given group at a time. Pathogenicity and lethality tend to be held in check except in individuals in a population that do not contribute to maintenance of the virus in the population, like the elderly and infirm who do not reproduce individuals vulnerable to infection and transmission. Why is COVID different from animals in these respects of populations? The answer may lie in that animal viruses establish carriers by preferring gastrointestinal infections that are not easily cleared and chronically shed transmissible virus. In other viruses, like influenza, especially in migratory birds and water fowl, it is predominantly a GI rather than respiratory virus, which most effectively maintains the birds as a reservoir rather than incapacitating or killing the birds, which would limit their ability to spread the viruses. The COVID virus has chosen a more unorthodox method to assure maintenance and transmission in the human population, although with time I believe we will find more and more asymptomatic GI shedders (by monitoring sewage which has begun) https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.25825 and https://www.medrxiv.org/content/10.1101/2021.01.08.21249379v1. It has chosen to enhance anti-parasite immunity like that used by the hosts to control parasitic worm, pathogenic protozoan and fungal infestations and infections. This response often controls the number of parasites to a tolerable, but not immediately lethal, level and prevents further infestation (a process called premunition), but does not totally eliminate the parasite. In children, this form of innate non-specific immunity often rapidly clears an infection without inducing long term immunity. Therefore, they are allowed to survive, grow and reproduce more naive vulnerable individuals after spreading the virus in the population. They are also vulnerable to re-infection as they grow older. Adults can mount this type of immunity but then develop specific adaptive long term immunity, but unfortunately also “memory” of the initial innate response with a vengeance. If this “remembered” non-specific response becomes overt or is activated, as it is highly vulnerable to do, by non-viral stimuli, it can lead to autoimmunity and pro-inflammatory nonspecific disease, which has been observed in “long haulers”. The fatal severe COVID is a continuum of the infection from inapparent widespread tissue infection to a late activation of this parasite immunity to the extreme, death, without a break. This type of incomplete immunity is beneficial for resisting parasites and in tumor immunology because it is highly effective locally, but suppressed systemically to avoid collateral damage to normal self tissues.
I have observed an artificial reproduction, perhaps enhancement, or at least a mimic, of this type of reactive oxygen species innate immunity early in my research career. I described it in my first book . “Even though weaker, nonspecific cytotoxicity was expected with glucose oxidase and horseradish peroxidase, they were used. Very malignant Novikoff hepatocarcinoma (including metastases) in rats, spontaneous mammary adenocarcinomas in rats, L1210 leukemia in mice, B16 melanomas in mice, and carcinogen-induced squamous cell carcinomas in hamster cheek pouches all responded to regional or local injections of the cross-linked enzymes in saline and glucose solution. The Novikoff hepatocarcinoma responses were 50 to 100% cures in animals treated. Lactoperoxidase could be substituted for horseradish peroxidase, and similar results were obtained. However, galactose oxidase substitution or the absence of either the glucose oxidase or the respective peroxidase in the preparation failed to bring about tumor regression. L1210 leukemia in outbred white mice showed 50% cures. Treatment of B16 melanoma prolonged life from 23 days postinoculation of controls to 37 days with treatment. However, no simple dose-response curve was demonstrated..Also, smaller squamous cell carcinoma tumors responded better (some with cures) than did larger cheek pouch tumors, which did not respond at all..No direct injury to normal tissue was observed in histopathological sections of treated animals. However, some animals with heavy tumor loads (P388 lymphoma, L1210 leukemia, some with Novikoff hepatocarcinoma) died more quickly when treated than did untreated controls due to an apparent “necrotic crisis” from dying tumor tissue.”— Type-B Cytochromes: Sensors and Switches by J.L. Kiel. https://a.co/aJEAVsl. I was acutely aware of the relationship between oxidase/peroxidase innate non-specific immunity and resistance to parasites and cancer because I entered Texas Tech University Health Science Center, School of Medicine, Graduate School, in the Departments of Biochemistry and Microbiology, as one of their first PhD students, in the summer of 1977 at Lubbock, Texas, with the intent to study this anti-parasitic mechanism. My dissertation research was on the cytotoxic mechanisms of peroxidases, a principle antimicrobial and anti-parasitic enzyme in granulocytes and macrophages of animals and humans. I wanted to study the effects of eosinophilic peroxidase on blood flukes (an animal counterpart of Schistosoma called Heterobilharzia americana) but my graduate committee and the safety officer would not approve of my keeping my infected snails in an aquarium in the laboratory. Therefore, I turned to peroxidase killing of cancer cells.
This highly localized approach is necessary because parasites and cancers disguise themselves as normal host tissue and this type of immunity must attack them without confusing them with normal tissue, which could be fatal or at least highly damaging to normal tissues and organs. It is a very delicate balance that could go either way. Therefore, any treatments or vaccines must direct a response that limits early replication of the virus and do not trigger an overt systemic parasite immune response. Hopefully, the current vaccines and treatments currently being evaluated will do this.
As a final personal note, I dealt, in my professional lifetime, with trying to address these mechanisms in other infectious zoonotic diseases and where infectious agents come from, go to between outbreaks, and how to stop them from re-emerging and spreading. By my measure, what has happened with COVID-19 would have been a total failure if it had been in my purview of investigative and applied functions and responsibilities. I spent the first third of my career investigating the non-specific responses to chemical, biological, and radiation insults, especially non-ionizing electromagnetic radiation, microwaves and radiowaves, and the second two thirds investigating means to detect hidden infectious agents and to stop re-emergence of infectious agents from between outbreaks. You may question my authority and knowledge in this area and assume I should have some honored and respected position in academia or industry after my retirement from serving the military and nation. I do not. It appears the arts and sciences of attribution and Counterproliferation of biological agents, natural or nefarious, are so specialized that there is no venerable honored academic or industrial positions or no longer governmental positions that meet with my qualifications. Since my retirement in 2011 and being turned down many times for academic positions, I have only been called on by the federal government when emergency situations required my services and was summarily dismissed when the crisis passed. However, when the crisis occurs, as with COVID, is when my talents are least but albeit still critically effective if heeded. I thought that even at 71, I might be valuable in sharing my experience, knowledge and insights with those who need to follow me in these pursuits, which I did in the military, but am not allowed to do now except by my books, past publications and currently this blog. I will continue as long as one person reads this blog and am able to continue.
With the rise of many mutations and variants, the questions arise: 1) will the current vaccines protect and stem the tide of the pandemic? 2) Will the vaccines drive, by selection pressure, the establishment of new more resistant, transmissible and/or pathogenic variants? 3) Will masks and social distancing still be required after vaccination? Variants which emerged in Brazil (known as P.1.), Britain (known as 20I/501Y.V1 or B.1.1.7) and South Africa (known as 20I/501Y.V2 or B.1.351) are now the globally dominant strains because of their apparently enhanced infectivity and transmissibility.
Current vaccines work against the UK B.1.1.7 variant without the E484K mutation. However, recent clinical trials by Novavax and Johnson & Johnson showed that their new vaccines were less effective in South Africa compared with the UK or US, probably because of the high level of virus carrying the E484K mutation. However, Novavax vaccine was reported to have a 60% efficacy in South Africa which is a good response, when compared to influenza vaccine responses of from 40-60 %. Studies have shown that people who have been infected with SARS-CoV-2 generate T cells that target at least 15–20 different fragments of coronavirus proteins. Because of natural variability, a population will generate a large variety of T cells that could attack the virus (https://reader.elsevier.com/reader/sd/pii/S1074761320305379?token=3775A68CFC8B8609E4A6753EF03F560FAF6F4B30D3B821B81F3A1CBF077E6DB8C53232C5B16ACCA1E569F0AE6C5368F3). As I mentioned in an earlier post, it is very hard for the CoVID variant viruses to mutate to escape cell recognition because of this T cell variation, The specificity of antibodies works in favor of variants. A recent pre-print shows a single mutation can defeat monoclonal antibodies against the spike protein of the virus and increased cell receptor binding, unfortunately a rare converging of properties in a single mutation. The mutation has been observed in a recent variant in California, CAL.20C viral variant from clade 20C, lineage B.1.429, that since November 2020 has generated multiple outbreaks and is undergoing massive expansion in California. This L452R mutation allows SARS-CoV-2 positive selection toward strong viral adaptation against containment measures that work on less contagious variants and against increasing population immunity against previous forms. The L452R mutation is at the leucine-452 position in the receptor-binding area of RBD (receptor binding domain) at the interface with the ACE2 receptor. Replacing it with arginine is anticipated to result in both a much stronger receptor binding and escape from neutralizing antibodies https://www.biorxiv.org/content/10.1101/2021.02.22.432189v1.full.pdf. Escape from two monoclonal antibodies has been predicted in a recent Science article https://science.sciencemag.org/content/sci/371/6531/850.full.pdf.
In a preprint published on 9 February, researchers found most T-cell responses to coronavirus vaccination or previous infection do not target regions mutated in two recently discovered variants, including 501Y.V2 (https://www.researchsquare.com/article/rs-226857/v1). Also, the vaccine made by Novavax of Gaithersburg, Maryland, a single-shot vaccine made by Johnson & Johnson of New Brunswick, New Jersey, and a vaccine made by AstraZeneca of Cambridge, UK, and the University of Oxford, UK are less effective at protecting against mild COVID-19 in South Africa, where the 501Y.V2 variant dominates, than in countries where it is now less common. AstraZeneca’s vaccine was only 22% effective against mild COVID-19 in a study of 2,000 people in South Africa, but the trial was too small and participants too young to draw any conclusions about any loss of benefit in protecting against severe disease. However, another recent paper compared the vaccine – induced neutralization of a less contagious version of the SARS-CoV-2 virus from last year (USA-WA1/2020), to the new variants Brazilian P1 and UK variant B.1.1.7 which gave results “roughly equivalent.” Geometric mean titers (GMT) of neutralizing antibodies against the USA-WA1/2020 virus, the UK B.1.1.7 variant, and the P1 variant were 532, 633, and 437, respectively. The GMT against three versions of the South African B.1.3.5 variant were less at 195, 485, and 331, respectively (https://www.medscape.com/viewarticle/947064).
A recent, yet to be peer-reviewed, study of men from 70-84 years of age, who died from COVID-19, increased from 5% of those who tested positive for the older variant, to more than 6%, if confirmed positive for variant B.1.1.7. For men 85 years or older, the risk of dying increased from 17% to 22% of those confirmed positive for the new variant. Therefore, the apparent increase in severity of this new variant has been limited in scope. It may reflect an increased viral load rather than a normalized increase in pathogenicity. There is little evolutionary advantage for a virus to become more pathogenic in a host in preference to transmissibility. This may happen only if there is a maintenance reservoir host in which the pathogenicity is less and from which the virus periodically emerges entering the host more vulnerable to lethality.
As to the third question, until the pandemic has subsided, even vaccinated people, including those who may have gotten upgraded vaccine for new variants, should continue to use masks, social distance, and, of course, continue to use good hand washing practices. Another early treatment to block viral replication has been discovered; a single pill of the investigational drug molnupiravir, when taken twice a day for 5 days, has been shown to eliminate SARS-CoV-2 from the nasopharynx of 49 participants in a new study (https://www.medscape.com/viewarticle/947061). Phase 2/3 efficacy and safety studies of the drug have started. The drug creates viral error catastrophe by inducing replication and mutations until the virus can’t effectively produce viable copies. This new early treatment and the non-pharmaceutical practices are necessary to decrease the total number of viruses in circulation, to greatly decrease the probability of establishing new variants even if they are more transmissible, and especially if those infected shed larger amounts of virus asymptomatically or symptomatically.
“No Apology for the Truth I apologize for any errors you may find in this collection; like all human endeavors, it is subject to revision, but do not let that deter you from finding Truth within.” What we did will echo in history, but not remembered for the bioattacks, epidemics, pandemics that never occurred,
Although One Health has come a long way since Rudolf Virchow, MD, in the 1800’s stated “Between animal and human medicine there are no dividing lines—nor should there be. The object is different but the experience obtained constitutes the basis of all medicine,” and coined the term “zoonosis” to indicate an infectious disease that is passed between humans and animals, it is still having difficulty in connecting in the transition between animal and human infectious disease, the “No Man’s Land”, until the crossover occurs. In 1947, James H. Steele, DVM, MPH, founded the Veterinary Public Health Division at CDC. He became the Veterinary Father of One Health. His lead produced nearly 70 years of Annual James Steele Conferences on Diseases in Nature Transmissible to Man (DIN) which have pursued the One Health concept in infectious disease. The COVID-19 experience and the apparent surprises it has given to the medical community and the isolation of the veterinary profession or at least its sideline position (my opinion) indicates we have a long way to go. I worked for 22 years in the USAF AFRL in the no man’s land between outbreaks of zoonotic diseases in the little supported, some consider impossible, field of attribution of both natural and nefarious sources of infectious disease. However CDC and other organizations are making active efforts spurred by COVID-19 to re-invigorate the One Health Effort. https://www.cdc.gov/onehealth/basics/history/index.html
“In 1885, Louis Pasteur administered the first rabies vaccine in a person, marking an important turning point in public health. Today, zoonotic diseases continue to be one of the biggest threats at the human-animal-environment interface. A One Health approach, with involvement from experts across sectors, is key to preventing and controlling zoonotic diseases that can have global consequences.
60% of existing infectious diseases are zoonotic
At least 70% of emerging infectious diseases come from animals (Ebola, HIV, influenza, and COVID-19)
80% of agents with potential bioterror use are zoonotic.”
@CDC_NCEZID and #WorldZoonosesDay on social media.
From: John Kiel Sent: Tuesday, February 06, 2007 8:41 PM
Cc: Kiel, Johnathan L Civ AFRL/HEPC Subject: Re: Pulse Article – Texas Tech University Health Sciences Center
Dr. Kiel,
I hope you enjoyed the previous issue of Pulse I mailed last week. I am looking forward to working with you!
Below you will find several questions regarding you, your job and how you arrived where you are in your life today. Please feel free to add any additional information you feel would be helpful. Once I have your answers if I don’t need further information I will draft the article and send it to you for your review. Our first draft deadline is February 19th.
Thank you again for your help!
Where are you from? I was born in Houston, TX and grew up there, although my Mother is British and I spent some summers as a child with my Grandparents in St Helens outside of Liverpool UK (UK is kind of my second home).
What other degrees do you hold? BS (Texas A&M, veterinary science, 1973); DVM (Texas A&M School of Veterinary Medicine, veterinary medicine, 1974); PhD (TTUHSC, interdisciplinary in biochemistry and microbiology, 1981)
Why did you choose TTUHSC? Originally, because of a wound healing research program at TTUHSC that I saw in an advertisement on a bulletin board at Indiana University, Kokomo, Indiana, when I was taking classes there in calculus, during my duty as a USAF Base Veterinarian on Grissom AFB, Indiana, Peru, Indiana; when I got to TTUHSC, the program was no longer in effect, so I shifted to the anti-tumor effects of granulocyte and macrophage oxidase/peroxidase systems.
Who did you study under? Johannes Everse (Dept of Biochemistry) and Stanley S. Lefkowitz ( Dept of Microbiology; I believe he is now at University of South Florida, Tampa, FL, on the faculty of the Dept of Microbiology and Immunology).
Describe your experience here. It was very intense and stimulating. I was among the first of the PhD students at TTUHSC and maybe the very first inter-departmental interdisciplinary student. The USAF demanded that under the Civilian Institutions Air Force Institute of Technology Program that I complete my PhD in 3 years; I did so with a six month extension (in 3 ½ years); I believe this might be some kind of record of a single subject PhD, much less a double major PhD.
What did you like or not like about the university and or your experience? I didn’t like the hail, dust storms and the tornadoes; I did like the small town atmosphere for my wife and children and the flexibility of the university in accommodating my educational needs as a USAF military officer assigned to a civilian university; I especially liked the Chemistry Department courses on the main campus and the highly intellectually stimulating environment of the Dept of Biochemistry at TTUHSC; I also enjoyed working with the Dept of Surgery in the Medical School; we gave lectures together to local AMA branches on venomous snakebite treatment (another one of my avocations—venomous snake herpetology).
How did you come to choose medical biochemistry and what drove you to get your PhD? Although I had been on faculty, after my graduation from the Vet School at A&M, as an instructor of pathogenic bacteriology, before going into the military, I thought that pathogenic microbiology was on its way out in the late 70s early 80s; boy was I wrong, with the advent of AIDS (HIV), and other emerging infectious disease, this attitude completely changed (after I graduated from TTUHSC); so I decided to look at biochemistry as a way to unravel the mystery of why white blood cells would make free radicals to kill cancer cells (or infectious agents, but I focused on cancer because that was where the grant support was coming from for my graduate advisor in biochem), when such free radicals probably originally caused the genetic damage that led to the cancer in the first place (and aging as well). In the long run, my interdisciplinary education and approach has led to many opportunities within my military and scientific career to see interactions among many militarily and medically relevant “stressor” interactions—radiation, chemical and biological.
What is your rank and/or title? I am the Senior Scientist for Counterproliferation (a Brigadier General Civilian Equivalent in USAF) for the Human Effectiveness Directorate of the Air Force Research Laboratory
What do you do for the Air Force and why do you enjoy it? I mentor and lead a research team and serve as the USAF’s senior advisor on preventing and countering biological warfare and bioterrorism attacks through non-medical means (not vaccines or therapeutics, although we have spin-off research in this area). I like working with a team, like the conductor of an orchestra with very skilled, mature researchers being the concert masters or first violins. I prefer the group approach as opposed to the individual investigator approach, although I also enjoy having young people enter our group. They come as summer students, post docs, or in collaborative graduate study programs with various universities. I also enjoy “making a difference” in the defense of my country and its civilian population (especially in the case of preventing bioterrorist attacks).
I noticed that your research varies considerably in topic. Is that a result of your job role or are you interested in a myriad of topics? One of my patent attorneys once said that I was a “consummate scientist” ; I am really just a person with insatiable curiosity and interested in learning anything new in science—whether it is biochemistry, microbiology, physics, astronomy or engineering—I guess I am just a generalist or at worst a megalomaniac.
Are there any unique experiences that you’ve had in life you’d like to share? In 2005, I traveled around the world from West (from San Antonio) to East through Dublin, Ireland; the Netherlands; Hong Kong; Hanoi, Vietnam; Korea; San Francisco; and back to San Antonio in 2 weeks. In my last 10 years, I have traveled almost every month. My wife says I have learned to like every place I visit (and especially the one I visited last). These experiences have made me greatly appreciate, and respect other peoples, cultures, and countries, and has led to many gratifying professional international collaborations and interesting experiences abroad. Someday I will write a book about it.
Dr. Kiel,
Thank you for getting this back to me so quickly. I wanted to run something by you. It seems to me based on your answers that I have come across a diamond in the rough.
In this issue of Pulse I am also writing a four page feature story on alumni of the Health Sciences Center who are working in uncommon avenues of health care. I have already started contacting graduates who I knew fit in that category and I believe after what I just read you would be perfect to include in this feature as well.
If you are open to this, I would like to look for another Graduate School of Biomedical Sciences alum to feature in our alumni feature section (the one page features toward the back of the magazine) and move you to my uncommon occupations article instead.
I know you are busy and travel frequently but I will be happy to work with you in any way I can. Because the feature is much more in depth I may have some additional questions.
Ok, I am sympathetic with those suffering from COVID fatigue, and understand how many people just want to forget this tragedy and return to “normal”. However, their previous insulation from such infectious disease and the lull in history it created, are not the historical “normal”, but an illusion of circumstances. This fact is the reason we must not relegate the COVID event to a dusty shelf and forget it as if it were an aberrant case, but use it as a knowledge base and motivation to prepare for future such potentially inevitable events, to mitigate their effects, and learn the circumstances that prevent such events from materializing into full calamities again. I will give several old examples and a new potential one which may emerge. First, the appropriate approach is not solely based on a single discipline such as epidemiology, microbiology, immunology, vaccinology, ecology, sociology, etc. but rather a team, cross disciplinary one. Next, let’s summarize what we have learned about COVID that might guide future responses and which might be exceptional to the disease. COVID is in many ways a typical animal coronavirus https://wwwnc.cdc.gov/eid/article/27/4/pdfs/20-3945.pdf: (1) it is both a respiratory and gastrointestinal virus; (2) it can be very localized to the upper respiratory tract or the GI tract and be resolved there by innate immunity (primarily Interferon) with little consequences (except for generating carrier states or subsequent re-infection); (3) the amount of viral inoculum predicts the degree of the severity of the subsequent infectious disease; (4) it can trigger an immune pathway more familiar in parasitic and fungal respiratory diseases as well as tumor immunology than viral and bacterial diseases; (5) if the first line of defense (innate immune response) fails and adaptive immunity must resolve the infection then the virus becomes distributed in many tissues including the central nervous system (brain) leading to severe or even lethal effects before the adaptive response kicks in and resolves the disease; (6) the severe responses originate with the anti-parasitic response being activated all at once in many tissues, making an effective local response into a severe to lethal generalized response; (7) not suppressing or resolving this generalized response post-infection leads to “memory” which cross reacts with other stimuli non-specifically leading to lingering long term illness; (8) SARS-CoV-2 more profoundly affects the old than young on average unlike animal coronaviruses which are more severe in the young, although the multi system inflammatory response in some children says this generalized collateral damage can occur in children from time to time; (9) the high transmissibility by airborne and physical contact from host to host (and the natural evolutionary drive of mutants toward optimizing this) in close groups of infected (particularly asymptomatic) carriers and susceptible individuals, but failure of long term and distance environmental and aerosol transmission, respectively, maintains the disease in a population indefinitely, and ultimately, endemically. This latter social problem, followed too late by isolation of infected individuals after symptoms and early transmission, leads to the coronaviruses’ continuous maintenance in populations at 10-15% on average but not more at a given time, preventing natural herd immunity and providing plenty of viruses to mutate and select for new dominant variants.
Several new and old measures have proven valuable in prevention and in treatment of early infection, but difficult to uniformly apply, that is, to convince the general population to sustain. Vaccination is very effective, but a sustained large susceptible portion of the population leads to abundance of virus and opportunities for mutations and selection for vaccine-resistant variants. Masking, limiting close contact and vaccination must be simultaneously widely applied or they will become ineffectual in ending the pandemic. It must be realized by the public that viruses do not replicate or mutate in the environment. They are static and decline in infectivity like a biological toxin until they have a host in which to replicate and select for mutations that further their replication. If this cycle is broken, they perish. Antivirals, like Remdesivir (https://jamanetwork.com/journals/jamanetworkopen/articlepdf/2777863/garibaldi_2021_oi_210112_1616042465.1957.pdf) and Molnupiravir (MK-4482, EIDD-2801) (https://www.merck.com/news/ridgeback-biotherapeutics-and-merck-announce-preliminary-findings-from-a-phase-2a-trial-of-investigational-covid-19-therapeutic-molnupiravir/) or monoclonal antibodies (https://www.nature.com/articles/d41586-021-00650-7) truncate the disease only if it is stopped early before the virus is widespread in the tissues, when and where immune-mediated inflammation causes severe disease and possibly death. There is also early evidence that vaccination can reverse chronic lingering effects of COVID, perhaps by shifting the immune pathway away from Th17 toward the Th2 pathway, but not toward Th2 cell produced Interleukin 4 (IL-4), IL-5, and IL-13, which up-regulate antibody production, not toward neutralizing IgG, but toward antibodies targeting parasitic organisms. IL-4 and IL-13 induce B cell switching to IgE (anti-parasitic but allergy yielding antibody) production. IL-5 is the principal eosinophil-activating cytokine, mediating allergic reactions. Immunization may prove to act like “desensitization” to an allergen with allergy shots or by clearing low-level sequestered viral infection (appropriate Th1 as well Th2 pathways).
Three new approaches have grown out of COVID research and development: (1) Gene-based, mRNA and DNA vaccines, which produce precise and effective immune responses, stimulating not only antibodies that block an infection, but also a strong T cell response which can clear infections even if they occur with vaccination before they can become apparent or severe, responding better to mutations, and probably eliminating chronic infections too; (2) a new way to discover drugs by investigating protein-protein interactions; and (3) wearable, wireless, cell phone and app connected diagnostics moving from non-specific illness diagnosis toward the goal of immediate disease-specific diagnostics https://www.laboratoryequipment.com/574395-3-Innovations-Fueled-by-COVID-19-That-Will-Outlast-the-Pandemic/.
A new drug from Pfizer appears to have great promise in truncating COVID. An investigational novel COVID-19 oral antiviral candidate,PAXLOVID™, significantly reduced hospitalization and death, based on an interim analysis of the Phase 2/3 EPIC-HR (Evaluation of Protease Inhibition for COVID-19 in High-Risk Patients) randomized, double-blind study of non-hospitalized adult patients with COVID-19 at high risk of progressing to severe illness. On 16 Nov 2021, Pfizer asked regulators in US to grant ithe drug emergency use authorization. Generic companies can start preparations for the product once they get a license, but have to wait for the regulatory approval before they can supply it. Pfizer claims late-stage trials showed the pill cut the chance of hospitalization or death for adults at risk of severe disease by 89 %. The trials evaluated data from 1219 positive cases across North and South America, Europe, Africa, and Asia. https://www.npr.org/sections/coronavirus-live-updates/2021/11/05/1052679112/pfizer-covid-pill-treatment
All the above are focused on the specifics of COVID but what can we learn from this experience, in general, that combines with older ones to stop new emerging zoonotic disease events leading to pandemics? In my previous writings, I have emphasized how infectious agents fill pre-existing niches rather than merely force entrance into a new host species or environment. It is true that the virus or other microbe must have the means to do this, have the right ligand to bind to the new host receptor or characteristics to survive and be available for infection in the new environment of the new host, but these are based on natural variation (mutations and altered gene expression) coupling with the new host and environment or a deviation in that environment, providing opportunity for first successful entry no matter how imperfect, a foothold, pathogenic ecology. I will give several past and present examples of infectious disease which will illustrate my point; first, my favorite, anthrax.
This disease arises sporadically around the world in every continent except Antarctica, with hiatuses of 30, 40, or more years and even in areas with no recorded outbreaks amongst grazing animals. Outbreaks are associated with wet springs followed by hot, dry often drought ridden summers and rapid disappearance with the onset of winter and cooler temperatures. It is usually very geographically confined and may jump in occurrence among non-contiguous sites. After reports that anthrax bacteria could be grown in the roots of plants in the laboratory, we attempted to see if this occurred under natural conditions in the field. In cooperation with Texas ranchers, we located carcasses of animals that had died of anthrax (confirmed by culture and isolation from samples collected from them) and let them remain in place for three years. No viable spores could be found in the soil around or under or in the carcass remains after three years. However, viable anthrax bacteria were cultured and isolated from roots of plants growing on the sites where the carcasses had deteriorated. Other investigators had found that the anthrax bacteria grew in the guts of soil nematodes. This experiment showed the non-infectious vegetative anthrax bacteria grew in plants (especially during the wet spring growing season) and converted to infectious spores when the plants were stressed or died during the heat and drought, releasing infectious spores into the surrounding soil ready to infect animals, especially if they fed close to the soil or dug it up looking for remaining vegetation to feed on. Therefore, environmental conditions, not just the presence of the pathogen, are required to infect an available, vulnerable host.
Another example is a changing microbe in an existing environment, altering the course of the infectious disease manifested. Tularemia is usually considered to be of two clinical types, Type A and Type B, associated with certain species and geographical locations. The first case of human tularemia confirmed by bacterial isolation and identification was reported in Cincinnati in 1914. Dr. Edward Francis, also from the US Public Health Service, established Bacterium tularense (fulfilled Koch’s Postulates) as the cause of deer-fly fever in 1928 and the bacterium was eventually named Francisella tularensis in his honor for his contributions. Most of the outbreaks reported in the United States are sporadic. Most cases are in the Ozarks in the Mid-West (between 2001 and 2010, Missouri (19%), Arkansas (13%), Oklahoma (9%), South Dakota (5%), and Kansas (5%)), and in the Northeast in Dukes County (Martha’s Vineyard, Nantucket Island, and Elizabeth Islands off the coast of Cape Cod), Massachusetts, the latter among gardeners and grounds maintenance people. Between 2001 and 2003, the prevalence of the bacterium in a large sample of dog ticks (Dermacentor variabilis) from Martha’s Vineyard was 0.7 per cent. Prior to 1937, there was only one case of tularemia on the island, related to contaminated rabbit meat from the Mid-West. However, after more than 20,000 cottontail rabbits were introduced from Missouri and Kansas into the Massachusetts’ mainland and Martha’s Vineyard and Nantucket Islands for the purpose of sport hunting, cases of tularemia (Type A) began to occur after a hiatus of several years. Every state except for Hawaii has reported cases at one time or another. There has also been a small concentration of cases in the Northwest and others localized in Northern California near San Francisco recently (between 2001 and 2010). Although the main source of tularemia is direct contact with infected rabbits or rodents, it can occur, in humans. through the bite of a mosquito or a gnat, from contaminated food or airborne dust which then contaminates water and/or food. Even though the microbe is rather fragile, the low infectious dose and maintenance in free living amoebas, Acanthamoeba spp., particularly in airborne resistant cysts, makes there environmental contamination widespread. In Europe, its source has been somewhat different (Type B). Tularemia was first recognized as a distinct important human disease in Europe following large water-borne outbreaks which occurred in the 1930s and 1940s in parts of Europe and the Soviet Union. In 1959, Russian researchers designated two subspecies, F. tularensis biovar tularensis (Type A), which is highly virulent in humans and animals, with its principal reservoir being the cottontail rabbit, and F. tularensis biovar palaearctica (Type B), the principal cause of human tularemia in Europe and Asia. It is mildly virulent in humans, but causes large scale, lethal epizootics in the principal reservoirs, the water rat and vole rat. The disease is manifested as ulceroglandular tularemia when entering the skin (which may be without breaking the skin), characterized by a cutaneous and tender regional lymphadenopathy. Percutaneous penetration may also manifest as glandular tularemia, regional lymphadenopathy without ulceration. Inhalation of Francisella tularensis bacteria can result in primary pneumonia, ingestion results in oropharyngeal symptoms of tonsillitis and/or pharyngitis with cervical lymphadenopathy. Other clinical types of tularemia include oculoglandular (infection of the eye) and typhoidal (fever with generalized but no local signs). Tularemia may vary widely as to severity based on the subspecies of F. tularensis subsp. tularensis, Type A being the most severe with a greater risk of death and Type B (Francisella tularensis subsp. holarctica also called palaearctica) being mild and self-limiting. At one time, Type A was considered confined to North America (the United States) and Type B in Europe (especially Russia and the former Soviet Union, where this Type B became the Live Vaccine Strain). Asia was known to have Type A (Francisella tularensis v. palaearctica japonica, Type B subspecies which has traits of Type A) and as such the antigen provided for human serological testing for diagnosing tularemia regardless of type. Only F. tularensis ssp. holarctica has been found in Japan. Tularemia bacterium is probably the least host specific bacterial agent known, infecting greater than 250 species of wild and domestic mammals, birds, reptiles, fish, in addition to humans and transmitted by a wide variety of arthropod vectors. The most common vectors are ticks, in the USA, Dermacentor andersoni (the wood tick), Amblyomma americanum (the lone star tick), and Dermacentor variabilis (the dog tick), which can maintain infection transstadially and transovarially. The most common insect vector is Chrysops discalis (the deer fly). The most common wildlife hosts include cottontail and jackrabbits, beaver, muskrat, meadow voles, and sheep in North America, and other voles, field mice, and lemmings in Europe and Asia. In contrast, tularemia is sometimes considered transmitted directly from an environmental, particularly, natural water source. This confusion has arisen because the more one looks at Francisella in the environment the more varieties, related species and strains one finds. Francisella is the only genus within the family Francisellaceae and is a gamma proteobacteria most closely related to Wolbachia persica, a tick endosymbiont, which begins to explain a lot. Based on DNA sequence and fatty acid composition, there are two species tularensis and philomiragia, with five subspecies of F. tularensis, tularensis, novicida, mediasiatica, and holarctica with a variant of holarctica from Japan which has the characteristics of a Type A rather than Type B Francisella. Philomiragia and novicida are considered the more likely waterborne environmental source forms, but this is in no way absolute in regard to the whole genus. Of these, only F. tularensis subsp. tularensis and subsp. holarctica consistently cause disease in humans, the others have caused disease on occasion under special circumstances. The source of the different levels of pathogenicity is not related to any toxin or clear-cut differences among the low pathogenicity and high pathogenicity species and strains. This ideal categorization has gone out the window. By surveying wild animals, feral cats and ticks in Houston, Texas, in 2005, we found Type B was endemic there and even in the air (found by Biowatch aerosol collectors). It was barely noticed in the human population because of its mild, self-limiting symptoms, but had been diagnosed there as far back as the 1950’s, but forgotten. Recently, Type B tularemia has appeared in Canada but now with symptoms more like Type A, muddling the separation. July 2018, a girl 4 years of age was admitted to the Health Sciences Centre at University of Manitoba for fever, right inguinal swelling, and dysuria. The patient’s symptoms had worsened in spite of completing a 5-day course of trimethoprim/sulfamethoxazole prescribed for presumed urinary tract infection but ineffective against tularemia (trouble with misdiagnosing this disease). The patient lived in a rural area bordering a forest in southern Manitoba, Canada. She had frequent contact with dogs and cats and often became infested with ticks. This and other cases caused by F. tularensis subspecies holarctica suggests that this subspecies might be more common in the Canada than the more virulent F. tularensis subspecies tularensis identified elsewhere in North America https://wwwnc.cdc.gov/eid/article/27/4/pdfs/20-3262.pdf. How can we predict such a change in the presence of a pathogen in a new previously unreported environment? Where to look? We found the answer in using an ecological tool called Geographic Information System (GIS). GIS is an “automated system for the capture, storage, retrieval, analysis, and display of spatial data” https://wwwnc.cdc.gov/eid/article/2/2/pdfs/96-0202.pdf. Common to all GIS is that spatial data are unique because they can be linked to a geographic map. The components of GIS include a database, spatial and map information and some mechanism to link them together. It has been applied to epidemiology since the 1990’s. We extended it to apply beyond a current outbreak to finding the microbe, the tularemia bacterium, in the environment between outbreaks. We used it to find a single infected feral cat in Houston.
Cultured and stained tularemia bacteria (Type B) from Houston, Texas, 2005.The complexity of tularemia diagnostics
GIS should be applicable to other zoonotic diseases before they emerge. The problem is finding the right data to input into the system.
Good data leads to good results with GIS
My last example is a virus that has the potential to bring back a scourge thought to be eradicated. This final example illustrates how an ecological niche can drive a microbe to fill it. Although it is difficult to test a simple model in an uncontrolled population like humans or animals in the wild, it can and has been demonstrated and predictive in at least one case that supports the validity of the model: the elimination of smallpox in 1977. This global experiment was based on a model assuming that if the proportion of the population that is immune exceeds the “herd immunity” for the infectious disease, then the disease can no longer be sustained in that population. In the case of smallpox, this level was exceeded by vaccination and the disease was consequently eradicated (helped by there being no animal reservoir). But was the ecological space it occupied also eliminated or did it become a vacuum to be filled? The problem is a related orthopox virus called monkeypox in Africa. Actually it is a rodent pox (from African giant pouched rats) that infects monkeys and subsequently humans, producing pox lesions very similar to smallpox. The pox viruses are closely related and widely distributed amongst mammals and birds. They can cross protect in immunity. A shipment of rodents from Ghana, imported to Texas on April 9, 2003, introduced monkeypox virus from West Africa into the United States. The same exotic animal importer introduced another emerging infectious disease previously, Viper Plague, from Ghana into the USA. It appeared to be a rickettsial disease, but later was found to be a co-infection with a rickettsia and a Type D retrovirus, associated with tick infestation, observed in vipers imported from Ghana. The disease had gross lesions very similar to Cowdriosis (Heartwater) a very important exotic animal disease not present in the United States but of great concern because of the potential damage it could cause in the US if it became established in native tick populations, and because it causes great loss (up to 70% lethality) in livestock (cattle, goats and sheep) in Africa. Viper Plague, which proved to be a mimic of Heartwater, and its tick vectors entered the USA in 2002. Tick control and tetracycline treatment of the snakes in prodromal or asymptomatic phases of the disease ended the initial outbreak. However, once signs appeared, it killed 100% of the snakes observed.
The rodent shipment that brought in monkeypox included rope squirrels (Funiscuirus sp.), tree squirrels (Heliosciurus sp.), African giant pouched rats (Cricetomys sp.), brush-tailed porcupines (Atherurus sp.), dormice (Graphiurus sp.), and striped mice (Lemniscomys sp.). CDC laboratory PCR and virus isolation showed two African giant pouched rats, nine dormice, and three rope squirrels were infected with monkeypox virus. Some of the infected animals were housed in close proximity to prairie dogs at the facilities of an Illinois animal dealer. These prairie dogs were sold as pets and then developed signs of monkeypox. The CDC and public health departments in the affected states, together with the U.S. Department of Agriculture, the Food and Drug Administration, and other agencies, prevented further spread of the monkeypox outbreak https://www.cdc.gov/poxvirus/monkeypox/outbreak.html.
Beginning in September 2017, Nigeria has experienced the largest monkeypox outbreak in the country’s history. By November 2019, it reported 183 confirmed cases across 18 states, yielding the largest outbreak recorded caused by the West Africa clade of the monkeypox virus. Genetic analysis indicates multiple introductions from animals into the human population. A viral sample collected in 2018 from a patient in Cameroon was genetically similar to a sample from Nigeria even though there was no epidemiologic linkage. This suggested an epizootic event covering the Nigeria-Cameroon border. This observation was in contrast to the performance of the West Africa clade, which tends to cause temporally and geographically isolated outbreaks. In addition , the 2017–2020 Nigerian outbreak showed a higher prevalence for adults (78% were 21–40 years old), in contrast to historical data of most patients’ being less than 15 years old. The changing demographics of this outbreak offers insights into the changing ecology of monkeypox in West Africa. Investigators have proposed two mechanisms for the resurgence after 40 years of no reported cases https://wwwnc.cdc.gov/eid/article/27/4/pdfs/20-3569.pdf. First, the populace experienced increased exposure to and interactions with forest animals, driven by deforestation, armed conflicts, and population migration. Second, herd immunity has declined because of discontinuing universal smallpox vaccination programs in the 1970’s. The illness typically lasts for 2−4 weeks. In Africa, monkeypox can cause death in as many as 1 in 10 persons who contract the disease. With increasing human to human transmission, the stage is set for a “new smallpox”.