What the USAF/AFRL Counterproliferation Team learned 1989-2011. What I continued as a contractor for USAF and DTRA 2011-2015:
“trying to define, or at least approach the value, as calculus would for an instantaneous velocity and trajectory, the timeless prediction of infectious disease emergence which defines pathogenic ecology as if it were a law of physics rather than an account of history.”
— The Black Dragon Trilogy by JOHNATHAN KIEL
https://a.co/91rCMnQ
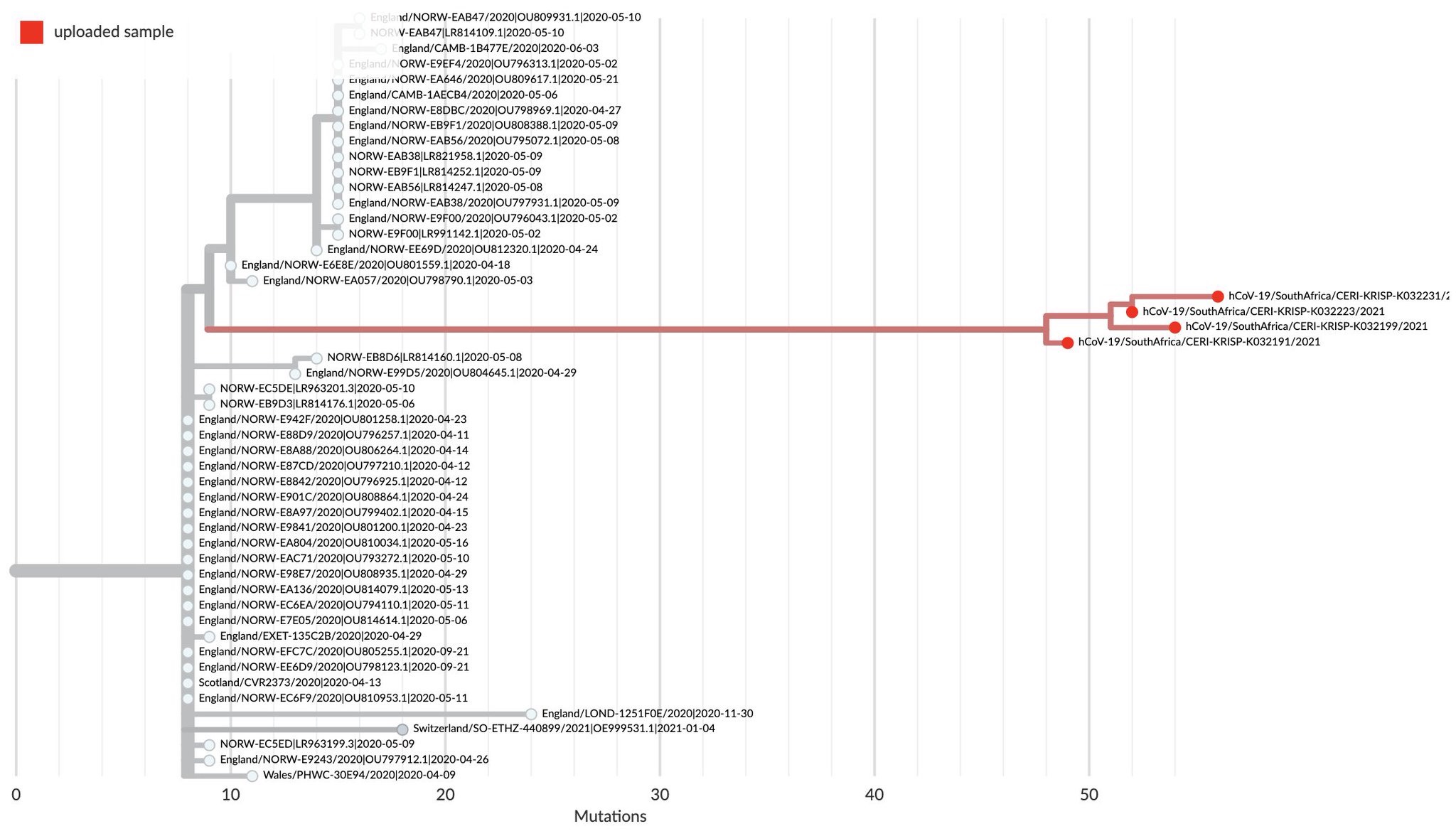
Detection and identification : Finding it early, very early: This is easier said than done because what is really required is finding the pathogen, or even worse, an emerging potential pathogen, before it emerges. For a well characterized pathogen, that has not genetically or phenotypically changed, this may be done with straightforward genetic testing like rapid PCR in the field or with an antibody-based test, like a lateral flow antigen test. But there is still a problem with sampling, so one does not end up with “garbage in, garbage out”, or worse an empty sample because what is sampled is mostly empty space in respect to the pathogen (appropriate sample volume). The problem is most boldly illustrated with the following statistical prediction of what it takes to find a positive at a given prevalence level of an infectious disease:
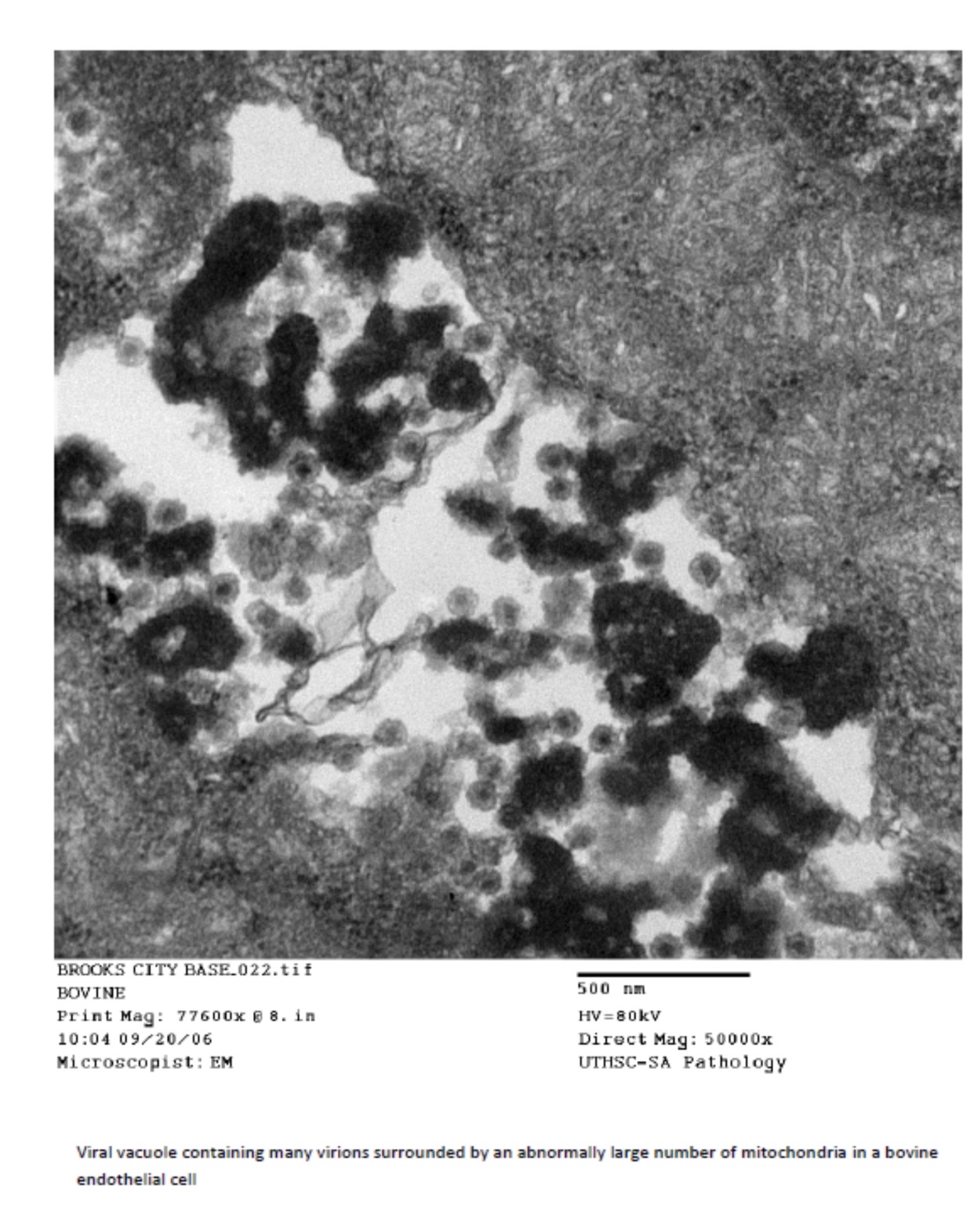
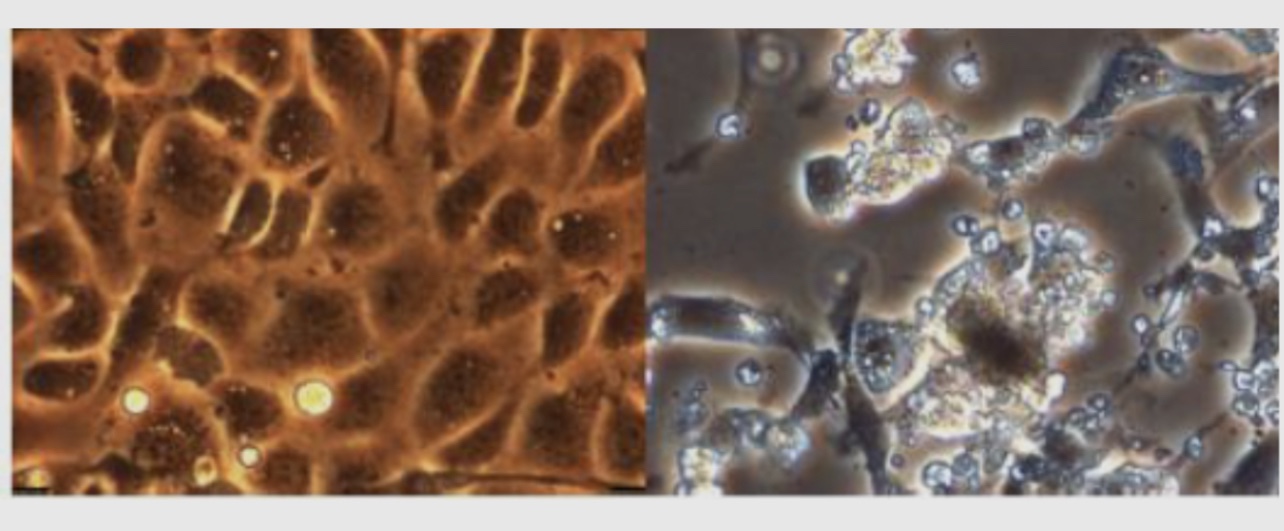
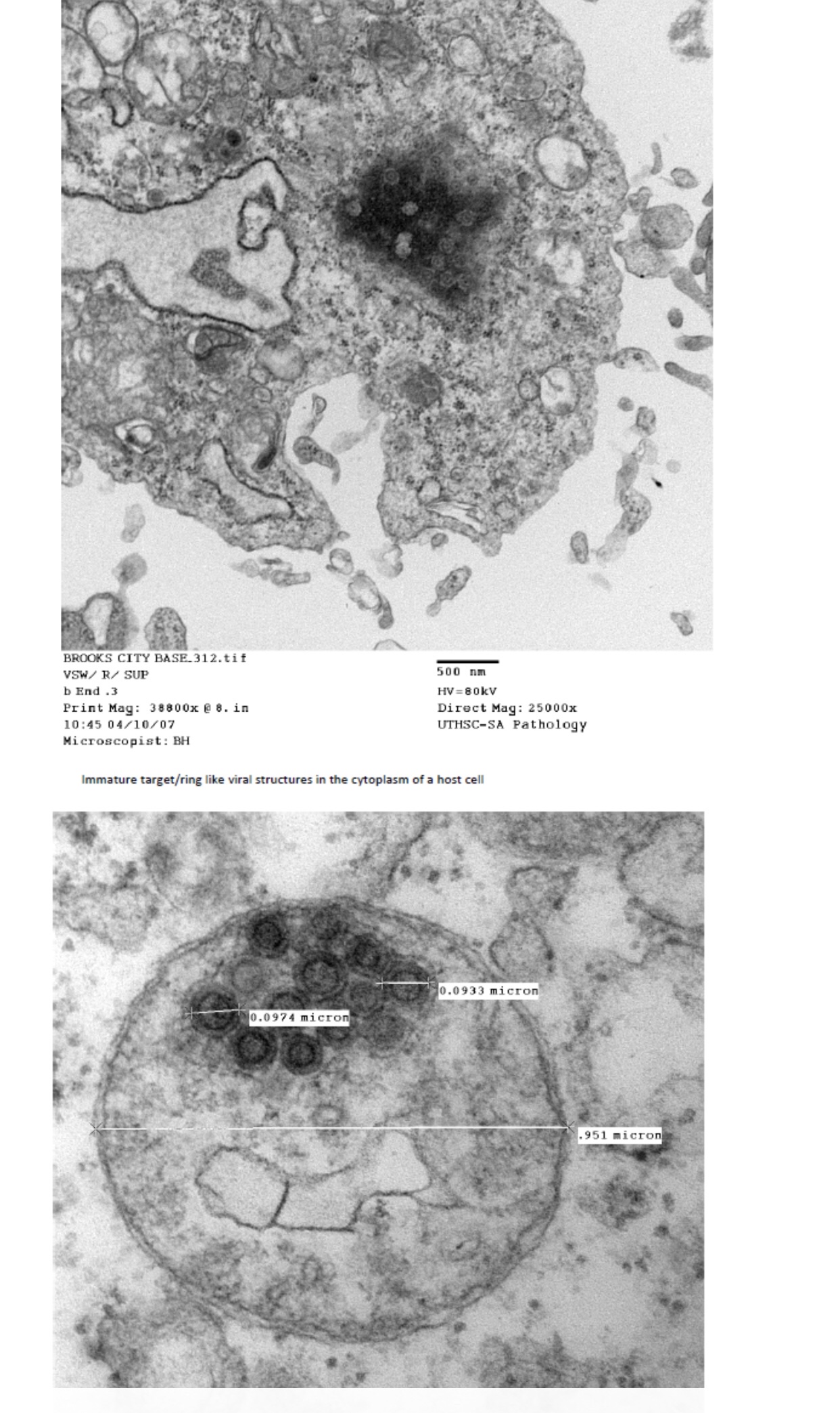
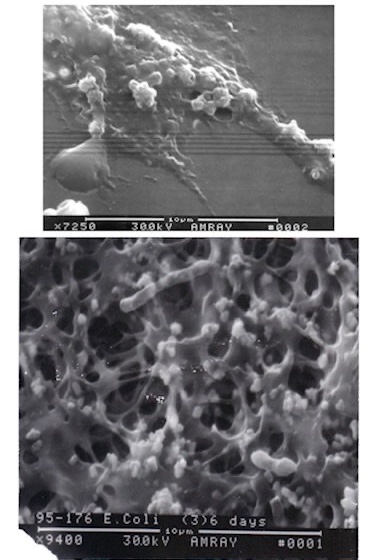
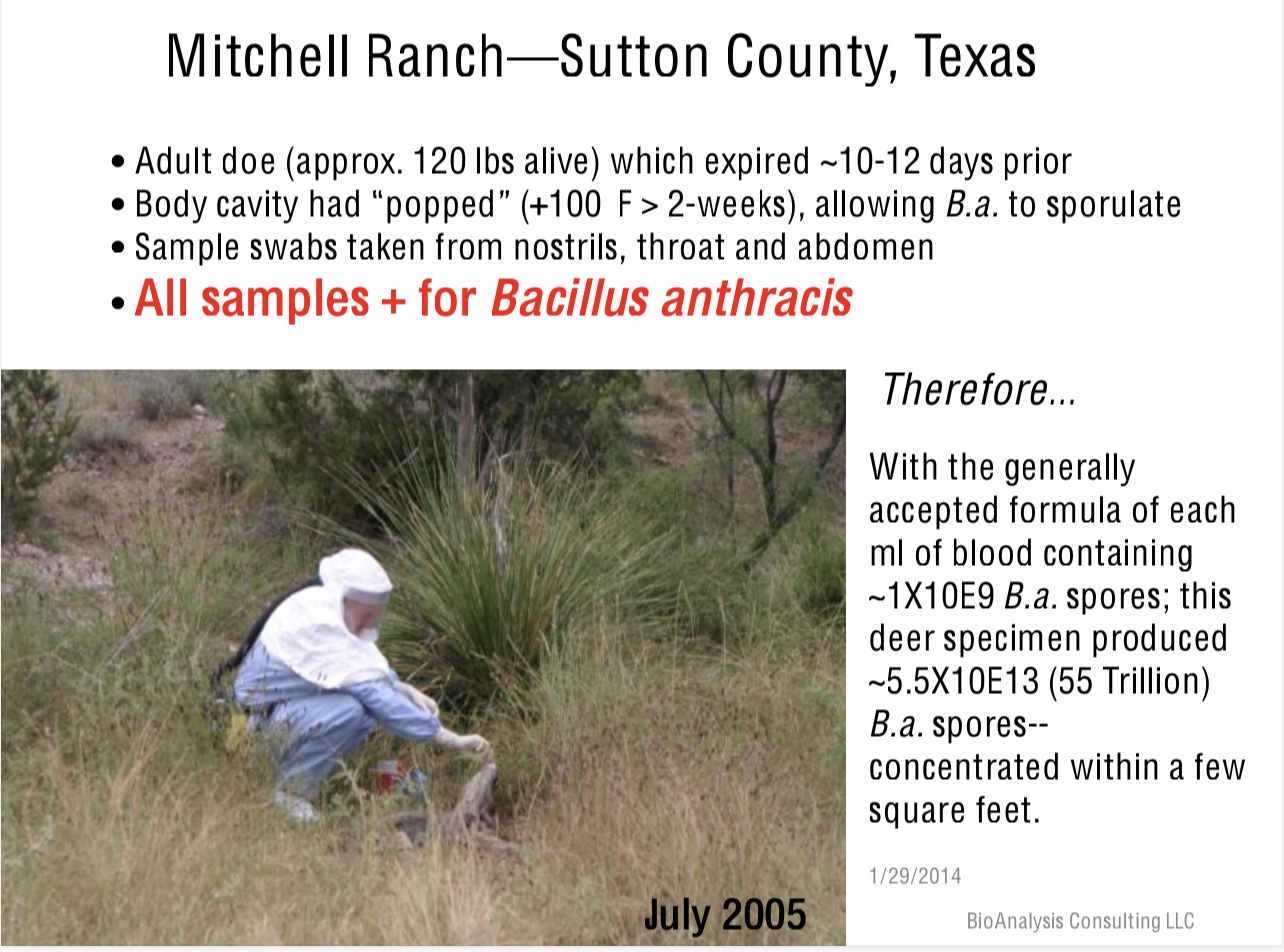
The above is a graph applied to sampling birds for avian influenza, in which the birds amplify the virus making it more likely to detect. When a microbe is diluted in air, soil, water or across surfaces, the sampling problem becomes more acute. These samples in which a pathogen or its toxin does not replicate will require concentrating and/or pooling of samples to find pathogens. This is why agents might not reveal themselves unless contact of a host is made with a naturally concentrated source or the rare event of contact with a susceptible host allows for replication and distribution to more susceptible hosts. Therefore, there is need for screening samples at the source with the appropriate assay to not merely collect “empty” samples and depend on statistics alone to find the pathogen. The key here is an appropriate assay: if it is too specific, a related but unknown potentially emerging pathogen will be missed, and if too broad, many non-pathogens may be detected and confound the analysis. The following pictures illustrate examples of these problems and attempts to solve them:


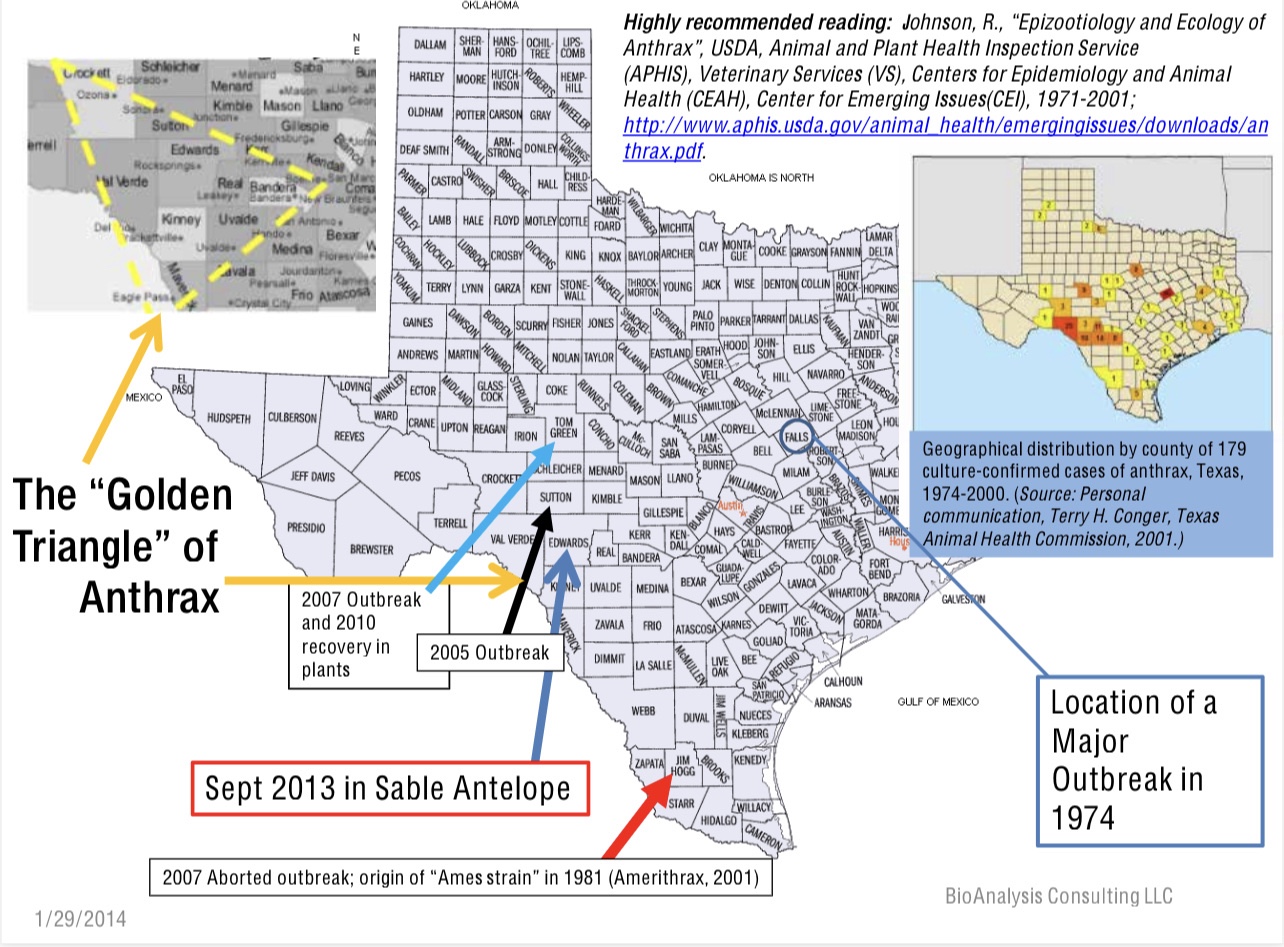
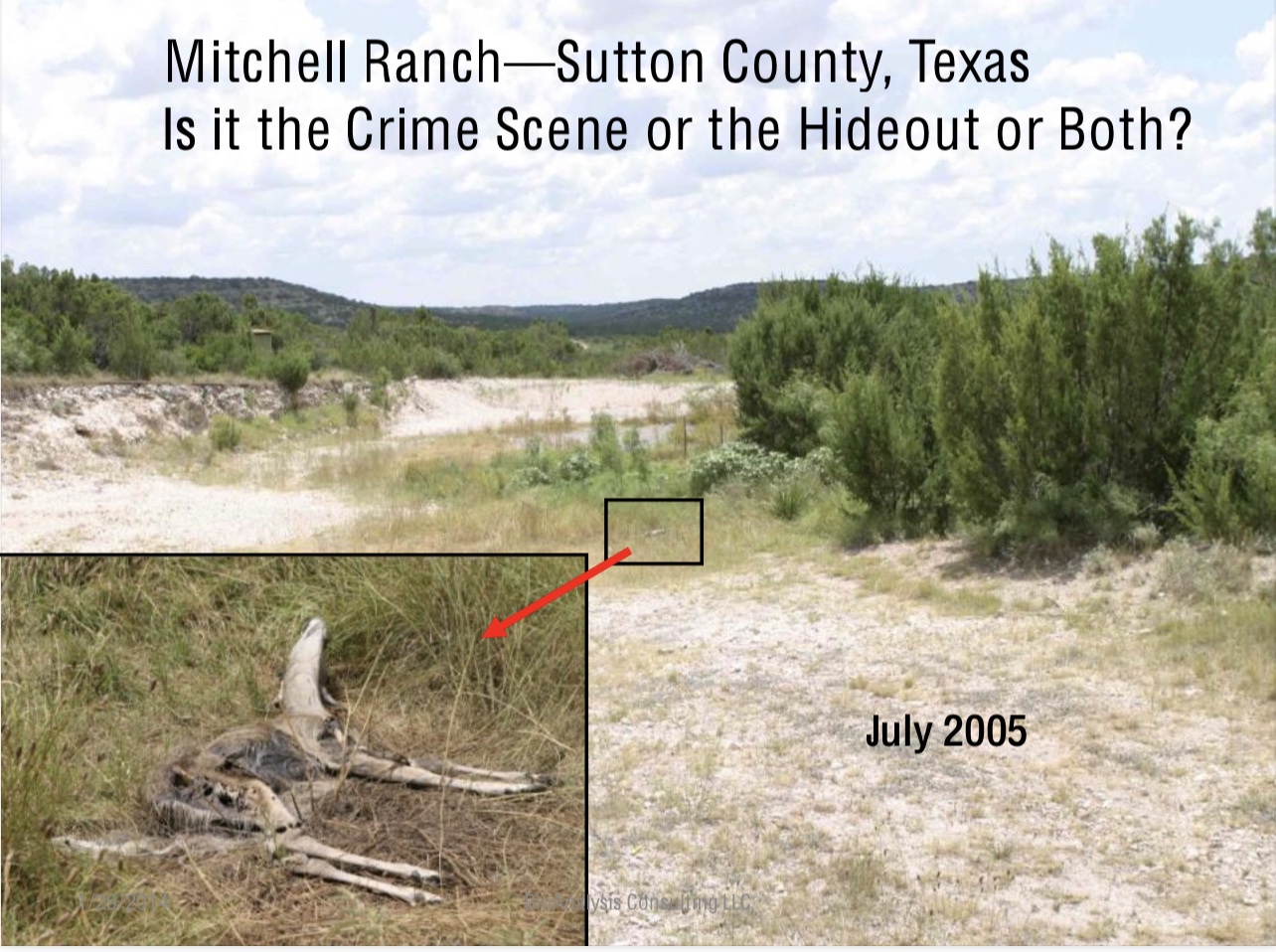
Knowing where to look: Lately, GIS (geographic information systems) models have become more useful in finding pathogens in the environment. However, one must know what parameters are required for the likeliness of the pathogens’ presence. As rapid whole nucleic acid sequencing moves out of the laboratory into the field and into the real time domain, confirming the presence of a pathogen in a sample will be more likely. However, for previous unknown potentially emerging pathogens, even a whole genome sequence may be necessary but insufficient for predicting pathogenicity. The following pictures illustrate examples of these problems and attempts to solve them:



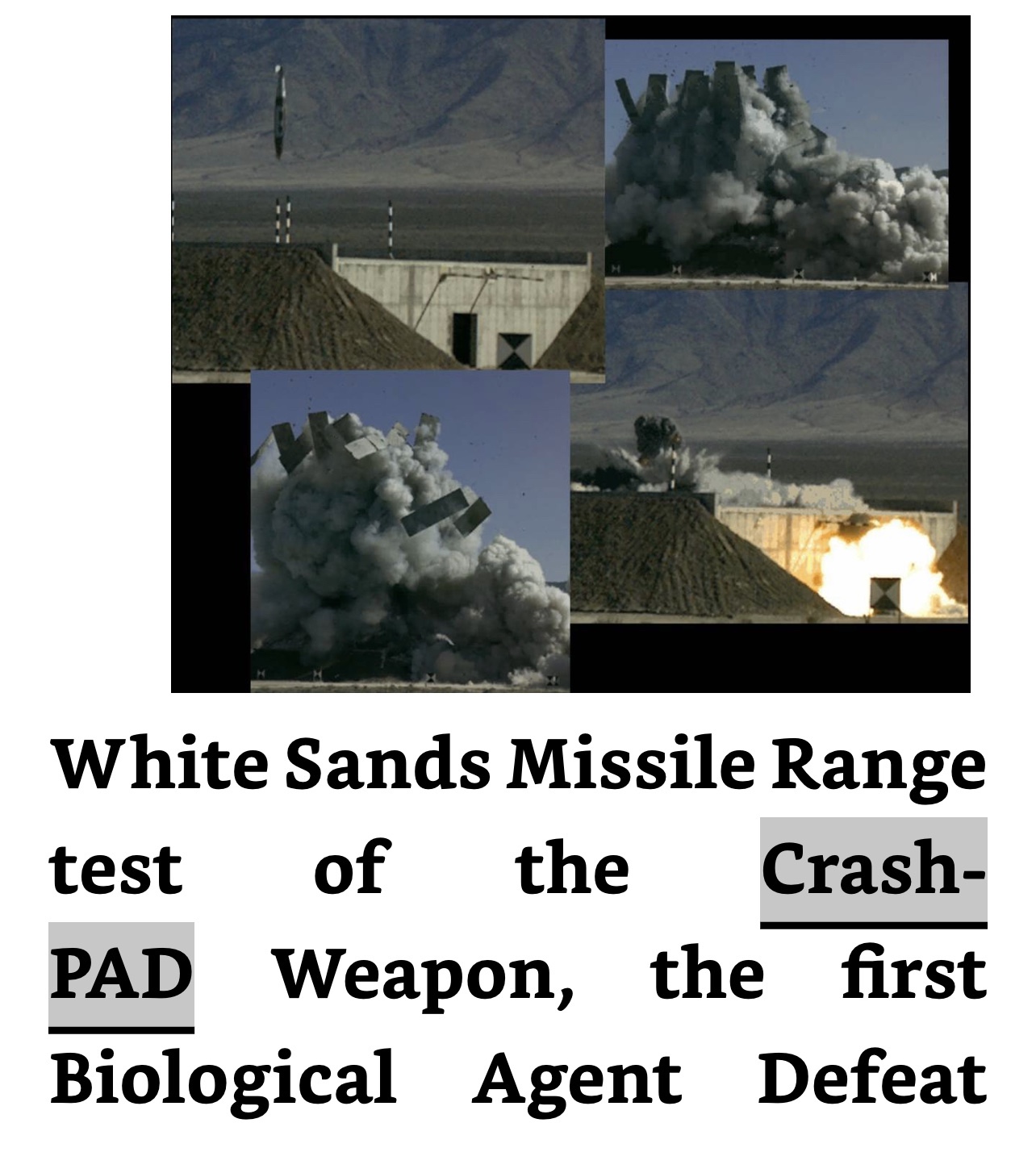
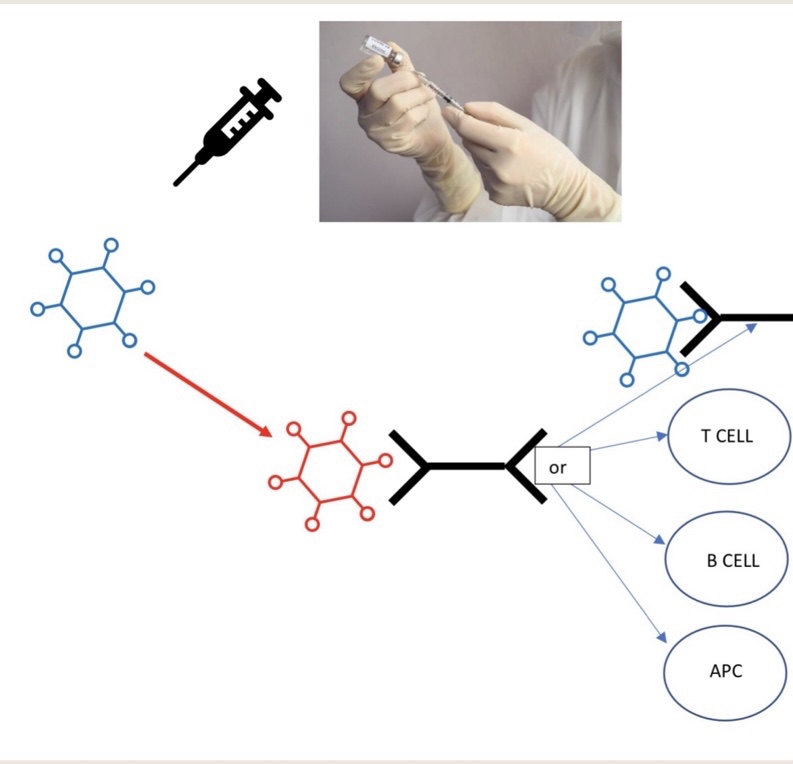
Knowing how to respond before mitigation is necessary: Once a potential pathogen has been detected, tentatively identified, and isolated in the field. Then, the next decision is how to respond. Should animal and potential human infections be identified and isolated or quarantined? How long and where? There are basically two types of bio defense, active and passive. The former is the essence of Counterproliferation (a corollary of the more general Active Defense against other Weapons of Mass Destruction), keeping bio agents in non-permissive territory, where there are political, territorial, and resource limitations. Passive and consequence management bio defense includes medical countermeasures like vaccines and pharmaceutical therapies and engineering and sanitary controls of infection. We are in this mode globally with COVID-19. This is more difficult and haphazard and less effective, but more likely to be supported because if the former is effective no one knows it because no epidemics or pandemics materialize. The production of influenza vaccines for different emerging strains every year is an example of rare anticipatory passive biodefense that has proven effective time and time again rather than the consequence management approach used for SARS-CoV-2 vaccines; albeit their development and deployment was in record time. However, the virus is still outrunning us with mutations leading to new Variants of Concern. Effective active defense is still a work in progress.

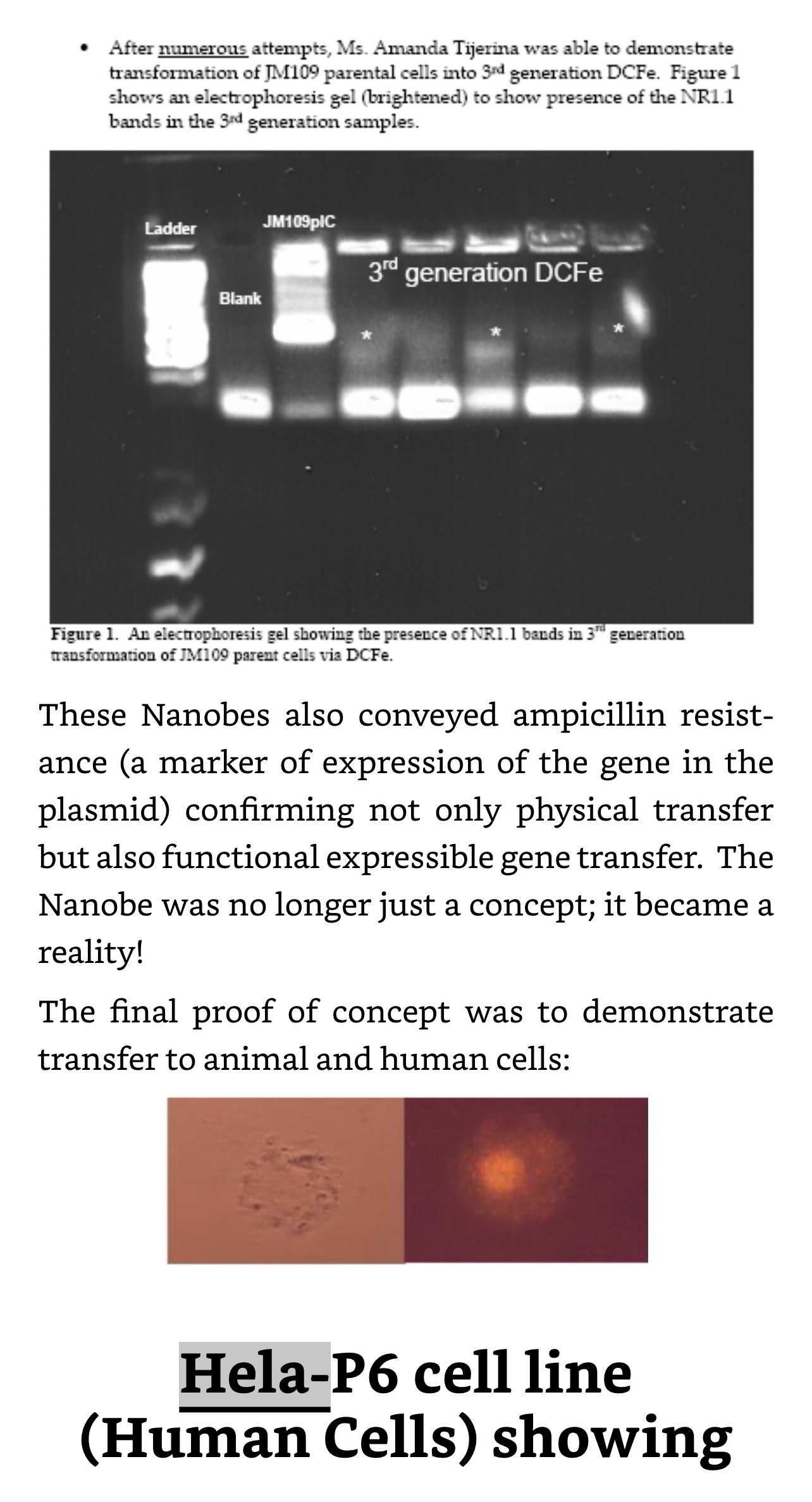
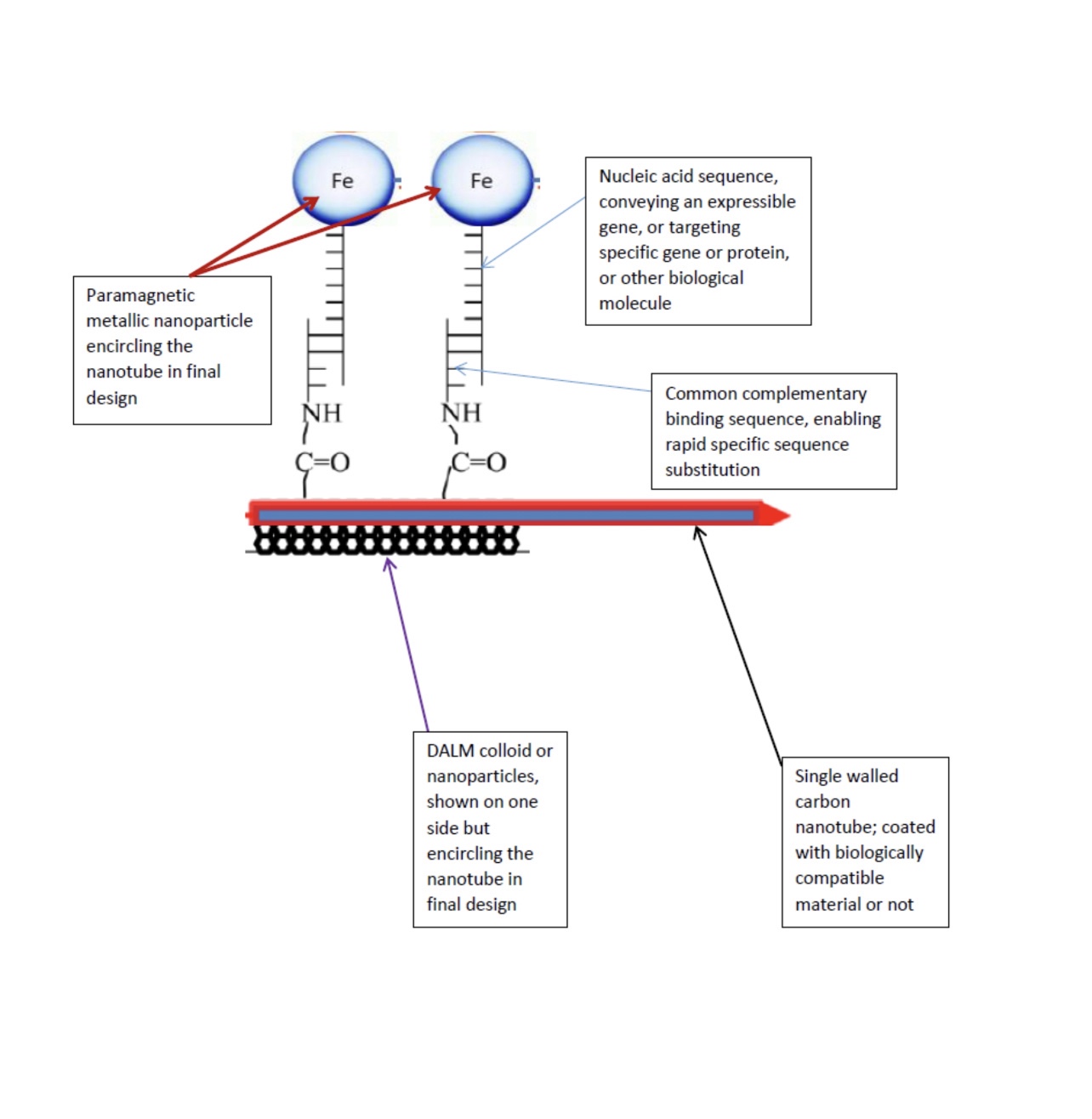
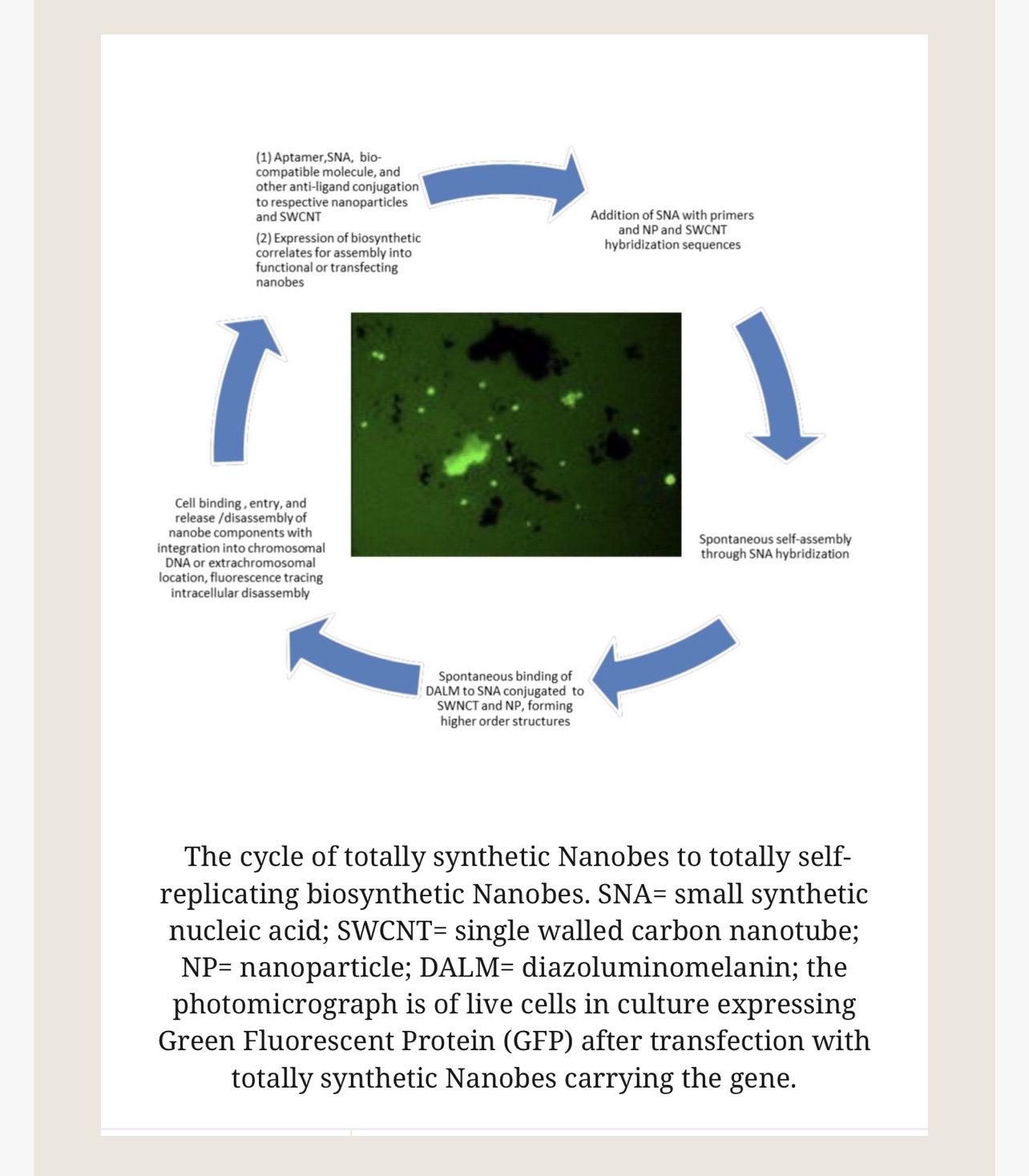
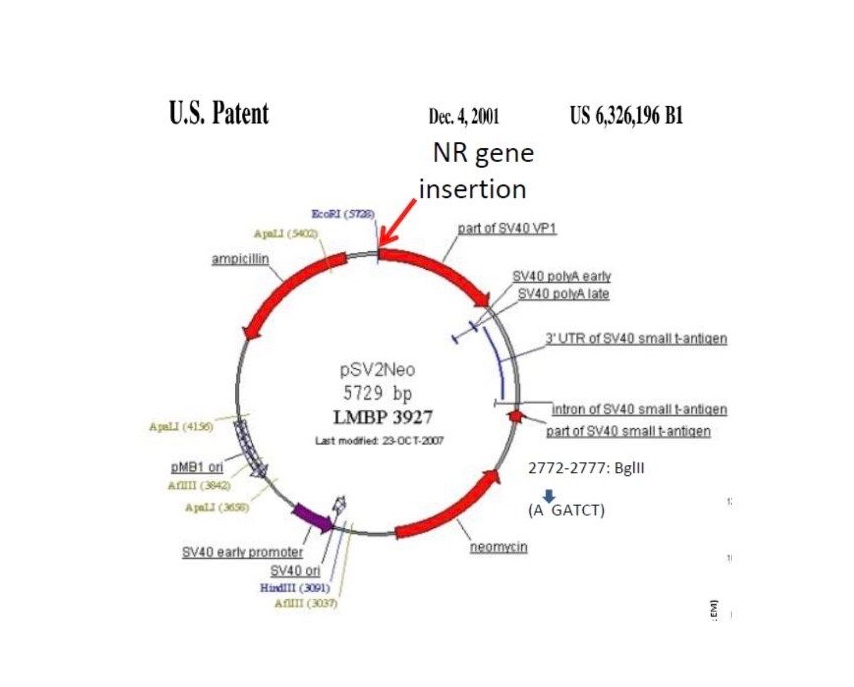
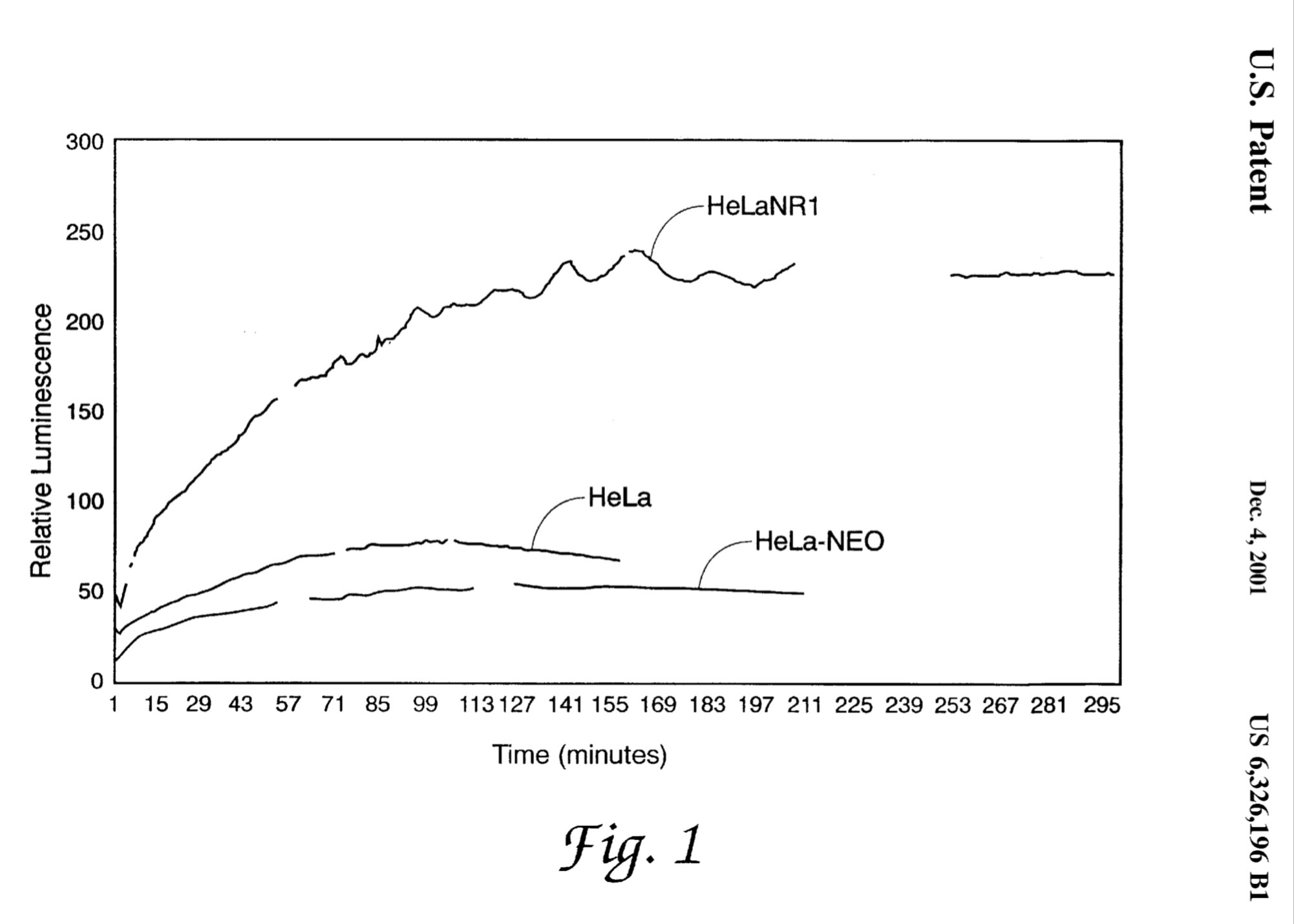
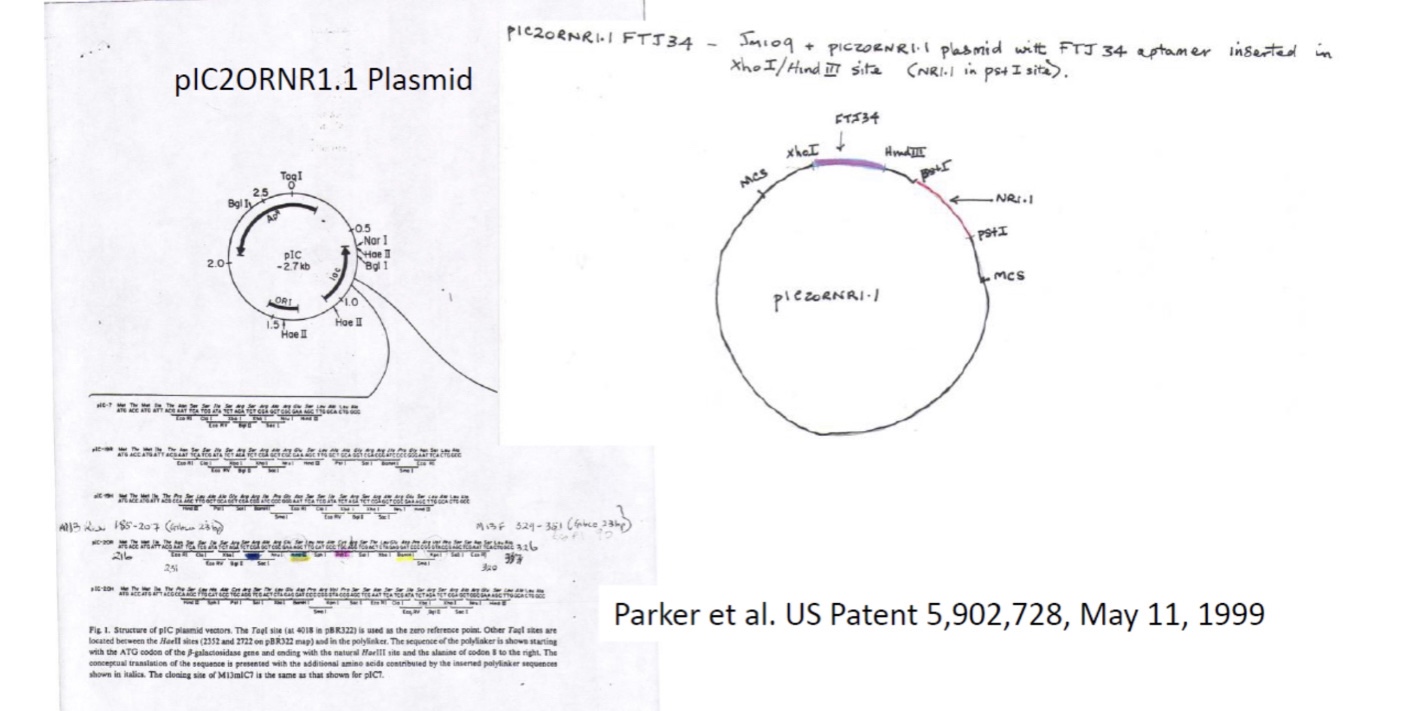
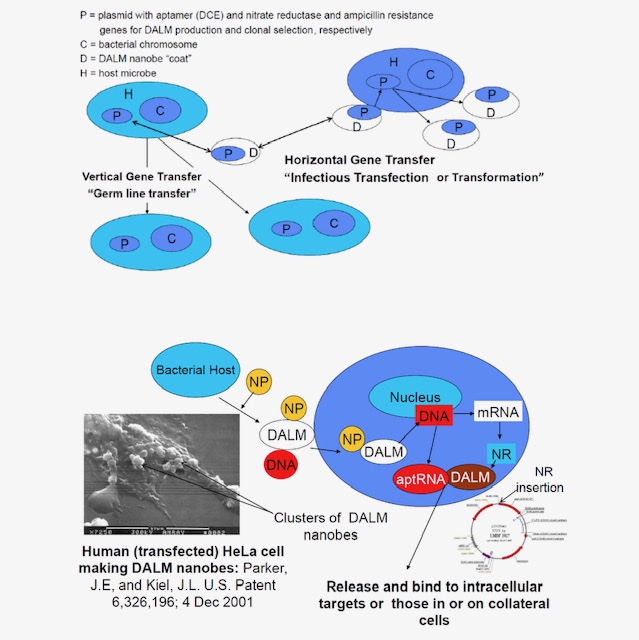
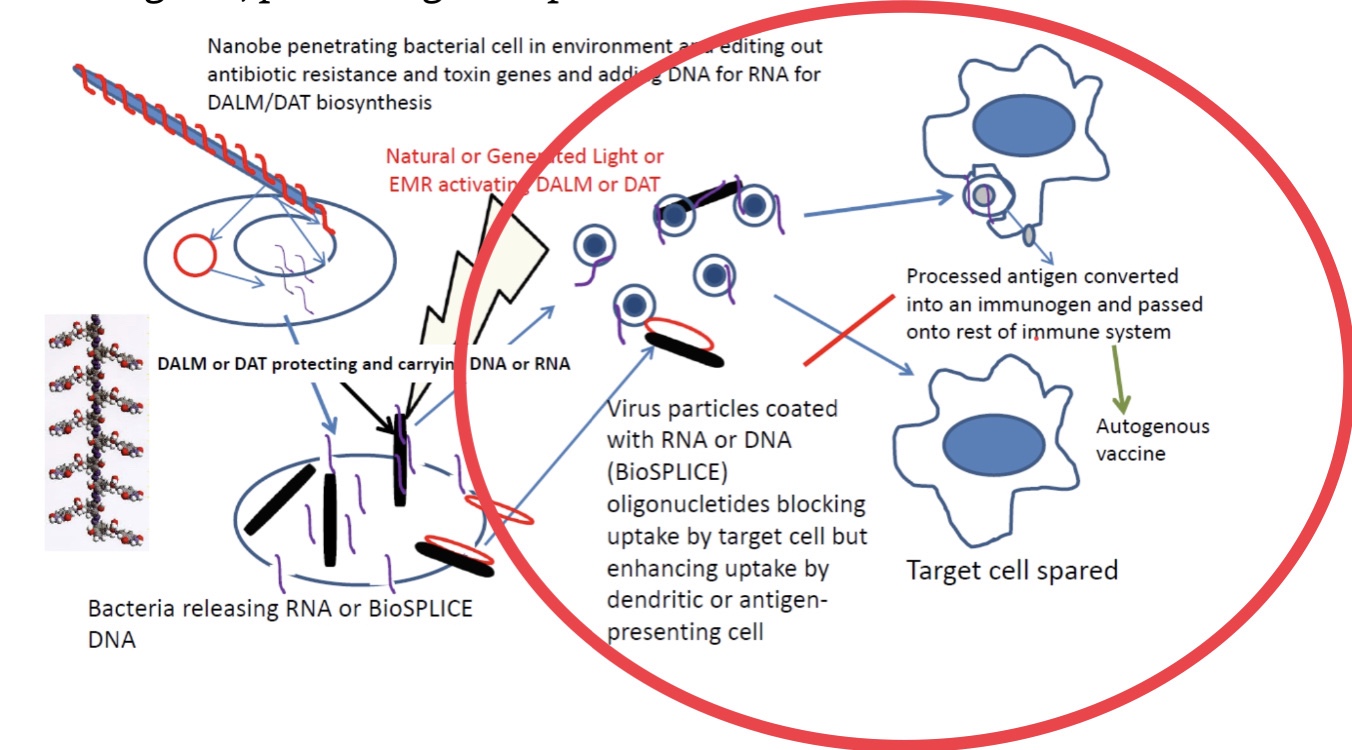
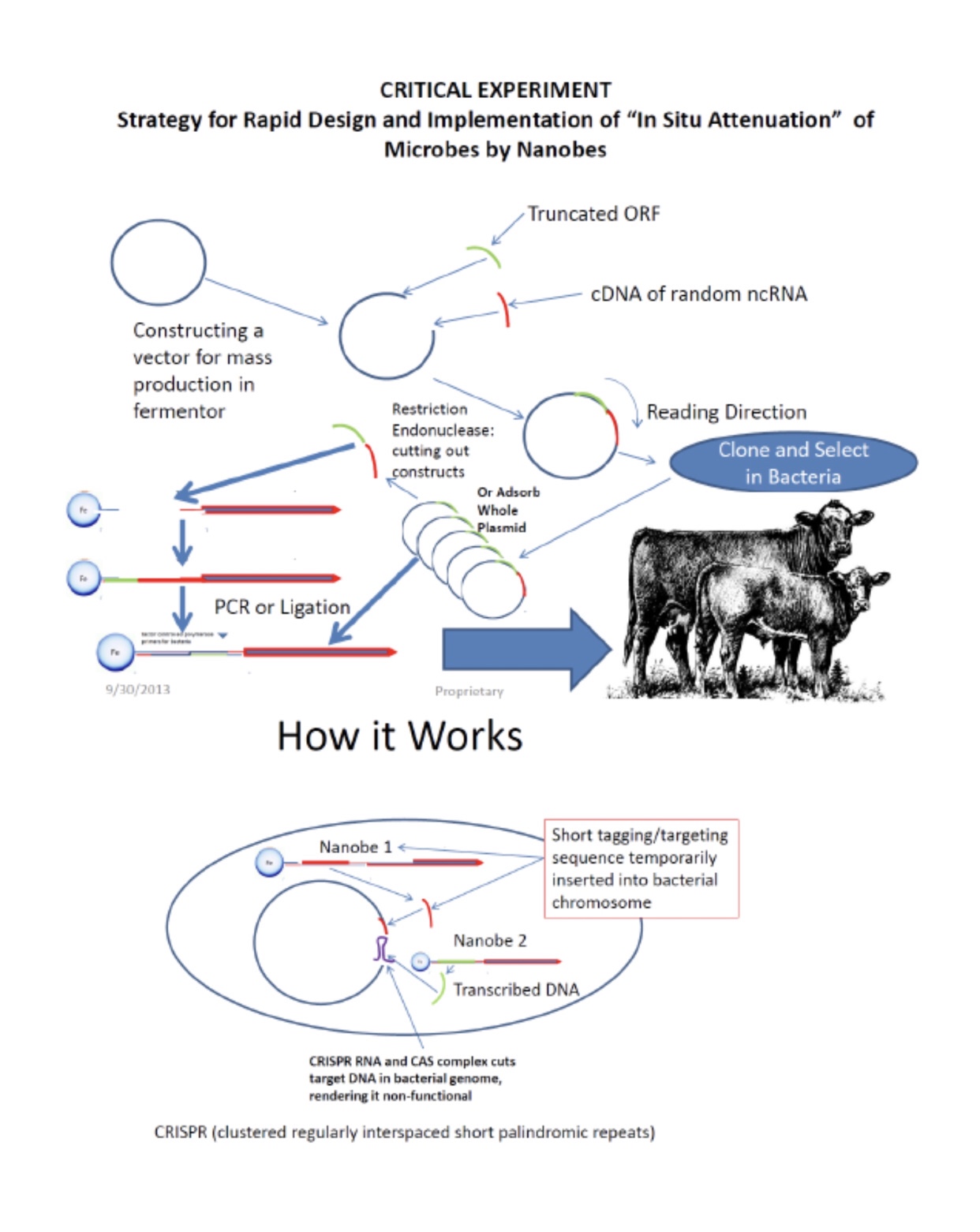
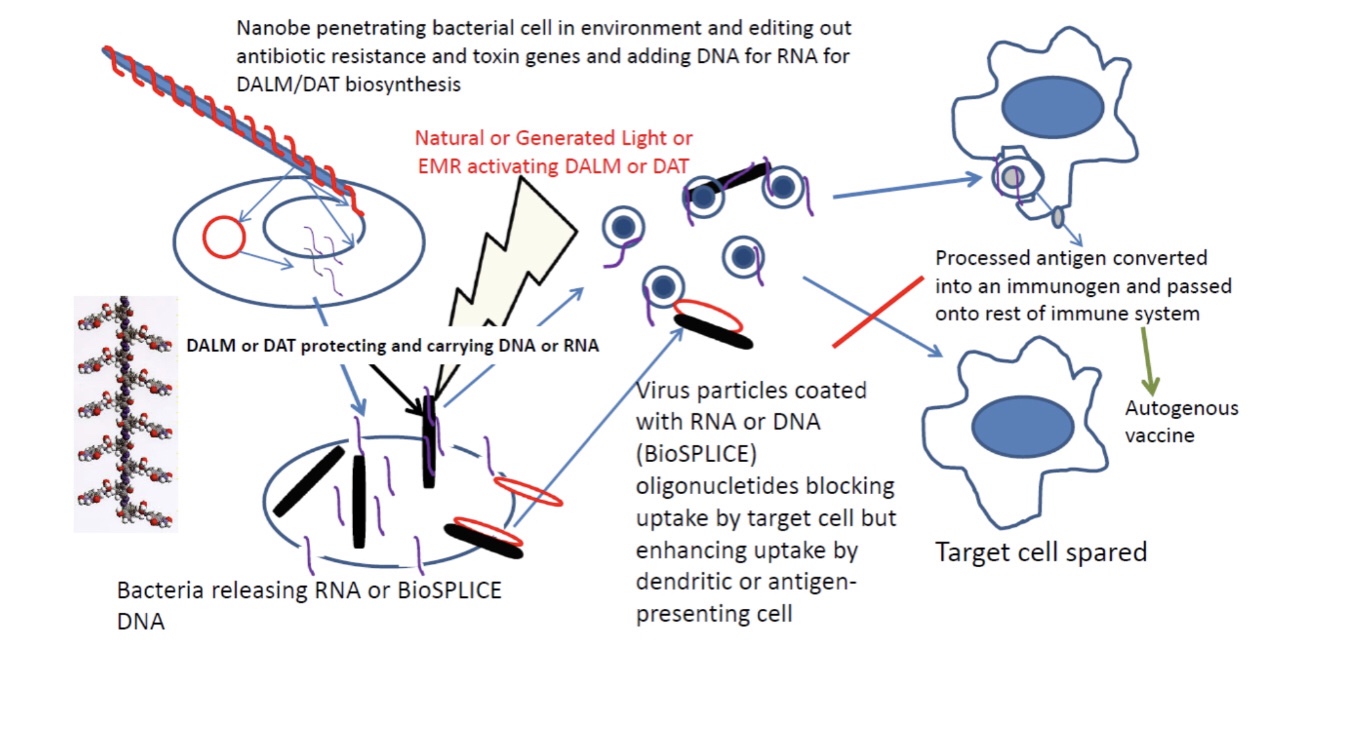
The Unfinished Solution for early active bio defense, closest to the point of origin, counteracting an emerging or re-emerging infectious disease before it becomes an epidemic or pandemic. The solution to which the AFRL Counterproliferation Team was finally led, as the ultimate goal, was the Nanobes. They were meant to be synthetically selected to detect, identify, isolate and kill specific biological agents seamlessly. An added objective was the biological replication of the Nanobes in the target microbe or cell infected with the objective virus to kill or make the respective pathogen susceptible to elimination.
“The Defense Advanced Research Projects Agency (DARPA) is soliciting proposals for the development and demonstration of advanced pathogen countermeasures, which will be a key component of DARPA’s overarching goal to remove the threat of biological weapons as a factor in the planning and conduct of U.S. military operations.” Really? And we hadn’t already done this? Now it is forgotten-“tears in the rain.”