It has become abundantly clear that testing for SARS-CoV-2, especially in the United States, is inadequate in amount and in timing. The military struggled with this problem years ago in the dilemma of “test to treat” versus “test to warn” in designing its detectors and diagnostics for biological warfare agents. The first was attainable but many times was too late: the phenomenon of “dead man walking”, the casualty alive but nearly 100% likely to die. The second was nearly impossible to achieve, with its instant diagnostics full of false negatives, and with no adequate immediate life-saving treatments to make it of value. This was the landscape we entered in 1989. We spent the next 22 years approaching the solutions asymptotically but our efforts were ended before completion because of change in priorities. Now we face the same problem under the COVID-19 crisis. To illustrate the severity of the challenge, we need to look no further than the number one biologic warfare/bioterrorism agent, anthrax. The following data illustrating this point and many of my previous posts, references and books have continuously emphasized these often ignored and postponed problems.
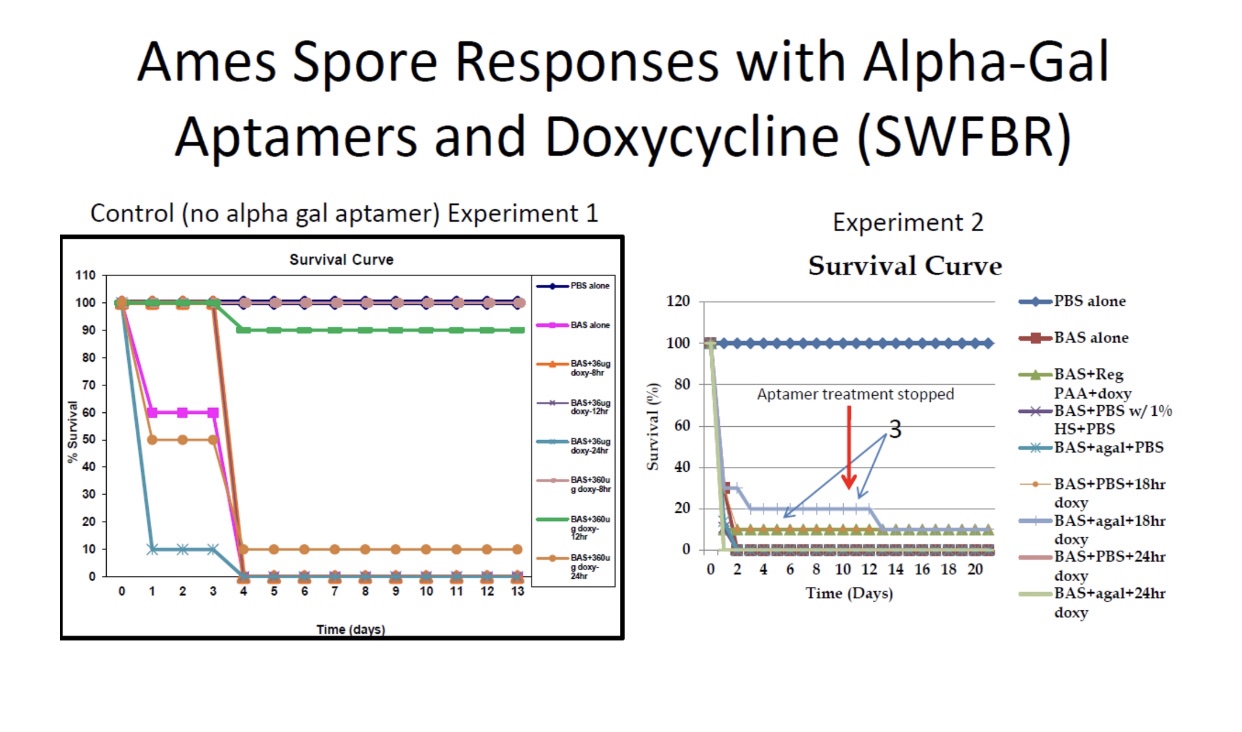
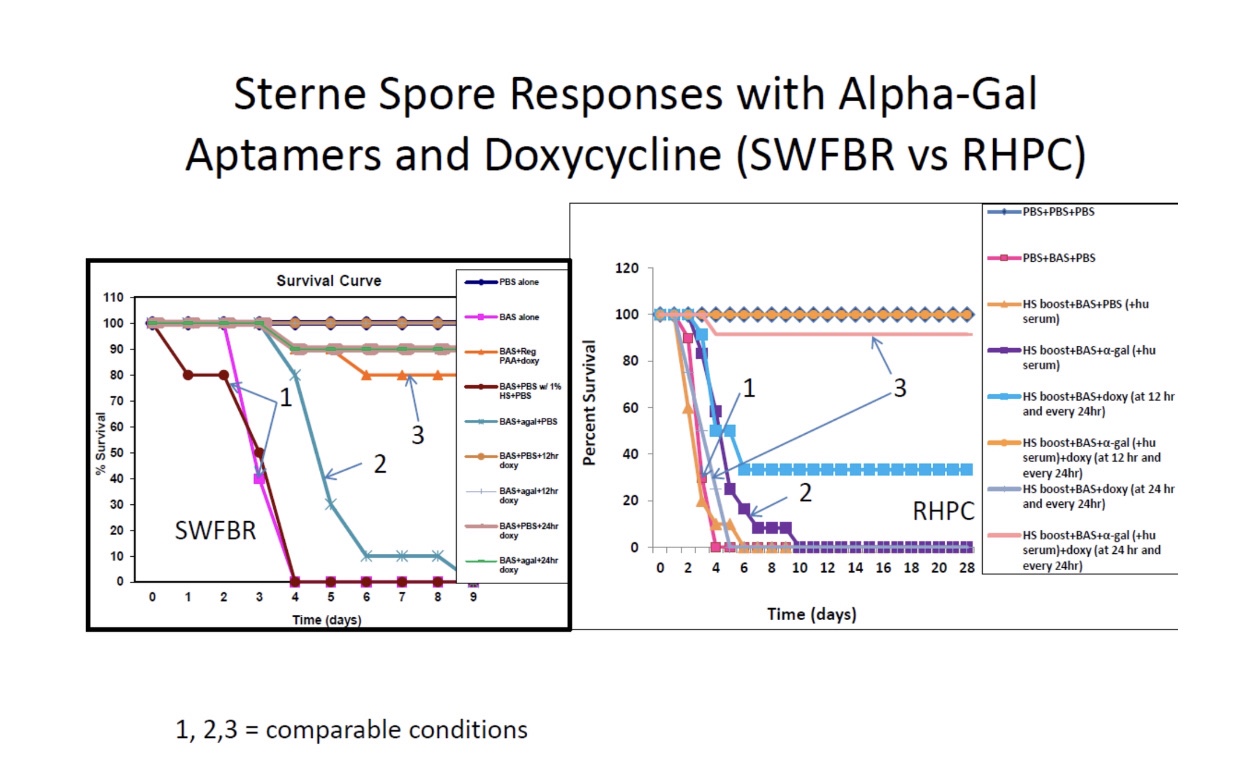
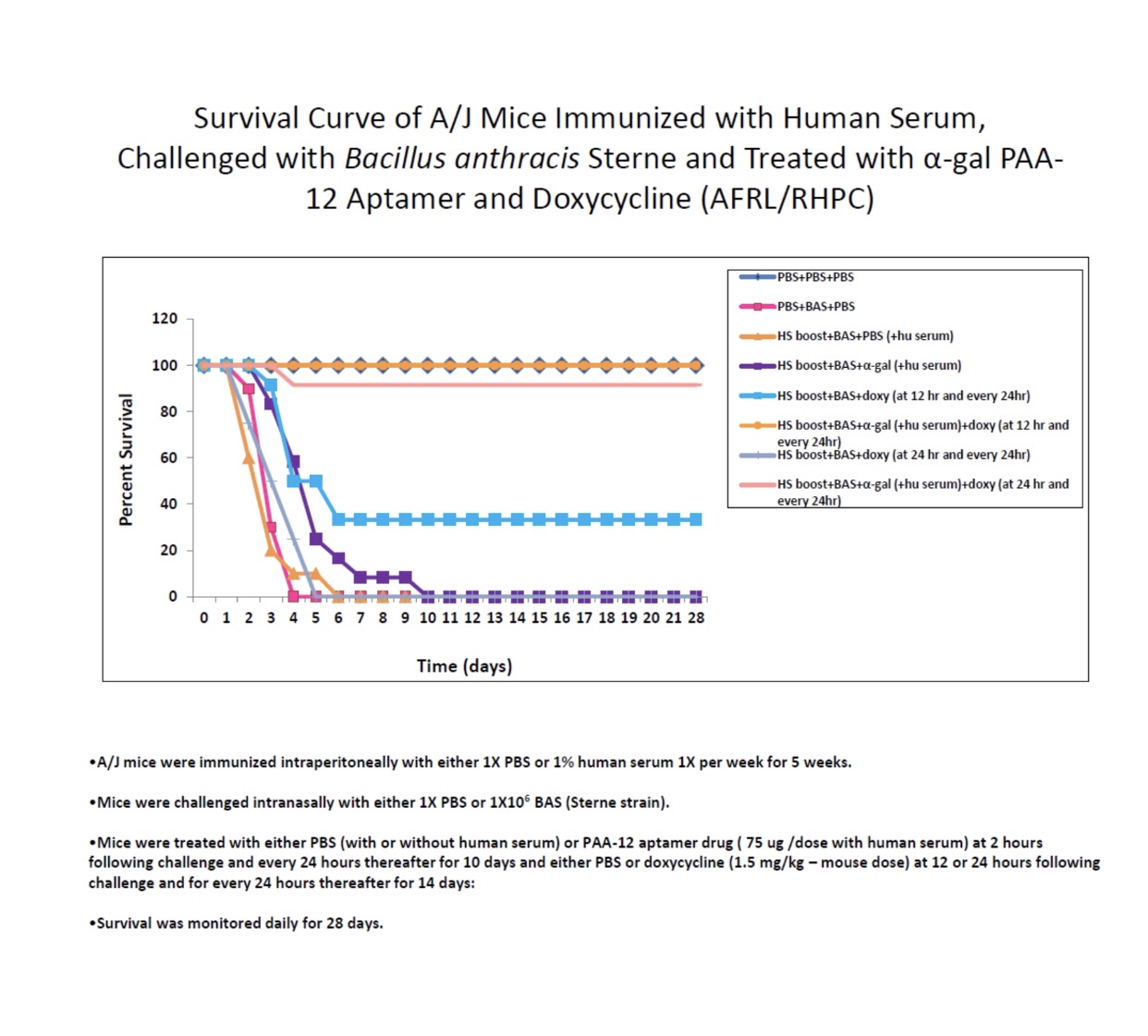
These graphs illustrate that antibiotics and other antimicrobial treatments must be applied early, at the appropriate doses, and for extended periods in the face of a highly lethal infection if they are going to have a significant effect or do more than delay morbidity and mortality.Another set of graphs that show inhalation or a lethal dose of anthrax spores has a critical period (2-4 days) in which treatment must be applied or it will lose all effectiveness; even with much less lethal COVID, the same principle of critical time window for treatment must be accomplished in order to avoid severe morbidity and mortality in individuals destined for those outcomes.These plots show how extreme the outcomes can be for a highly lethal infection like anthrax even for essentially the same treatments based on different protocols of dose and timing as well as combinations of treatment; even in a much less lethal infection as COVID, these types of responses become evident in the history of more severe infections, making prognosis very difficult for the apparently same treatments in different patients.The above circular chamber was the experimental test device to demonstrate the magnetic capture of biological agents on paramagnetic nanoparticles. The illustration below the chamber is of the fluorescent detector for the microfluidic chamber.This prototype proof-of-concept device was replaced by the following commercial device with modifications. The portable field device, built by Charles River Labs, flown and tested by NASA aboard the International Space Station, that was modified for biodefense. The graphs show the fluorescence detection by the device using a protein, thrombin, and a small molecule (nucleic acid base, nucleoside, adenosine) as targets representing pathogens and toxins.The multichannel microfluidics chamber and electronics of the CRL device. It was totally self-contained so that once the sample was injected into the channels, the biological agent(s) could be captured on the paramagnetic nanoparticles, detected by turned-on fluorescence, and kept isolated, alive and safe in the chambers to bring back to the lab for further analysis and even culture. The released artificial DNA or the agent’s released DNA or RNA (destructive analysis) could be amplified in a downstream chamber by isothermal amplification or PCR for more specific orthogonal identification. This process could even be used with random double-stranded DNA aptamers with primers to select and amplify selected aptamers to unknown agents to take back to the lab for further characterization and scale-up manufacture.These pictures show the near instantaneous fluorescent detection of anthrax spores by nanoparticle-aptamer-fluorescent dequenching compared to a field immunochromatographic lateral flow “home test”.As illustrated above, the detecting and identifying nanoparticles can be translated into biological agent killing particles for the environment: in the air or on surfaces, or if bound to biocompatible, non-toxic particles such as biosynthetic DALM or polymer made from the amino acid aminotyrosine, can be used inside the infected host, even self-administered by inhalation. They could even be used to genetically transform the biological pathogens into agents more vulnerable to other antibiotics and antimicrobials.
In conclusion, we now face a global pandemic and an assault on the USA, which if it were a strategic intentional biological warfare attack would have achieved its military objectives of mass casualties, overwhelming the medical and public health systems, economic damage (industrial capacity to wage war), causing panic, chaos, and internal strife, and compromised military readiness. For the sake of other priorities, we neglected our preparedness and abandoned our technological edge and advantage. The result 13,383,370 cases and 276,235 deaths in US of COVID as of this posting.