
Author: Dr. Johnathan Kiel
The Complex Immune response in COVID-19 May be Tied to Factors Released from Activated Innate Immune Cells
“Antioxidants, such as 3-amino-L-tyrosine, protect cells from the oxidatively induced death process. Concomitant with this increase in cell death and release of protective factor (altruistic factor to protect bystander cells from death signal) is an increase in spontaneous nitric oxide production by …cells. Although NO (nitric oxide) has been seen as an immunosuppressive agent based on inhibition of mitogen-driven lymphocyte proliferation, it may activate lymphocyte differentiation and lymphokine production. Evidence for the latter conclusion is found in the fact that TNF-alpha production goes up (pro-inflammatory cytokine that can cause cell death and shock) when human peripheral mononuclear cells are activated with NO. This effect could have been the result of gamma-interferon production. Further evidence for NO immune stimulation is found in the fact that expression of IL-2 (cytokine needed for specific immune response of T cells) in CD4 + T lymphocytes increases with NF-kappa-B expression (a gene expression inducer), which follows NO stimulation. Human peripheral blood mononuclear cells, monocytes and lymphocytes, have been shown to be activated by NO, as revealed by increased NF-kappa-B-DNA binding activity, enhanced rate of glucose transport, enhanced membrane-associated tyrosine phosphatase activity, and this activation, in turn, activated src family protein kinase p56lck activity in these cells (protecting against self-programmed cell death leading to proliferation and activation of functions)….The NO induces membrane component clustering similar to that induced by antigen binding to lymphocyte cell membranes and actin polymerization induced by hydrogen peroxide and hemin. The resolution of these paradoxical effects of NO may be based not only on concentrations but also on feedback mechanisms (which could prevent serious collateral damage or, if fails, permanent damage or even death).—Type-B Cytochromes: Sensors and Switches by J.L. Kiel
https://a.co/dNRlIiH
Sent from my iPhone
HeLa NR1 Cells which Can Be Used to Study Longterm Effects on Human Mucosal Epithelial Cells by Nitric Oxide Mediated Inflammation, Similar to Such Nonspecific Inflammation Expected with Severe COVID-19
www.atcc.org/~/ps/CRL-12510.ashx
Thanks to the contribution and sacrifice made by Henrietta Lacks, a Black America Woman, and her family, on the behalf of medical science and the American people. Henrietta was unaware she was the source of these cells from a cervical carcinoma biopsied during her treatment at John Hopkins Hospital in Baltimore, Maryland, in 1951. The cells were then grown by George Otto Gey, isolating the cell line known as HeLa, the most useful cell line for biomedical research and precursor of the genetically engineered HeLa NR1.
HeLa NR1 ATCC® CRL-13011™ is the only human cell that constitutively produces Nanobes. It is handled at Biosafety Level 2 because the cell line contains papova and SV40 viral DNA sequences. Biosafety Level 2 Cell Cultures are handled as a potentially biohazardous material under at least Biosafety Level 2 containment. These cell lines are associated with human disease, hazards include: percutaneous injury, ingestion, mucous membrane exposure (U.S. Government Publication Biosafety in Microbiological and Biomedical Laboratories). These cells have NOT been screened for Hepatitis B, human immunodeficiency viruses or other adventitious agents, unless otherwise reported on the Certificate of Analysis. Regardless of results reported on the Certificate of Analysis Universal Precautions according to 29 CFR 1910.1030 should be followed at all times when manipulating these cell lines. Biosafety classification is based on U.S. Public Health Service Guidelines, it is the responsibility of the customer to ensure that their facilities comply with biosafety regulations for their own country. Customers located in the state of Hawaii need to contact the Hawaii Department of Agriculture to determine if an Import Permit is required. A copy of the permit or documentation that a permit is not required must be sent to ATCC in advance of shipment.
The following is a scanning electron micrograph of a HeLa NR1 cell producing biosynthetic DALM nanoparticles (clusters of white nanoparticles being exuded). The cells’ ability to horizontally transfer genetic material through these Nanobes has never been measured. The added capability, if it exists, may have therapeutic research value or be an additional hazard in handling this cell line. The Brooks Counterproliferation Team never got a chance to investigate these possibilities because they were disbanded with the closure of the Brooks AFRL facility.

Specific Anti-flammatory which Inhibits White Blood Cell Oxidative Burst, Peroxidase Activity and Nitric Oxide Production which May counteract the Principal Cause of Severe Lung and Other Tissue Damage in COVID-19
In my graduate days, I discovered a compound, 3-Amino-L-tyrosine, which is a non-competitive inhibitor suicidal substrate of peroxidase and nitric oxide synthase. These are key parts of innate immunity that kill viruses, bacteria, fungi and parasites but can cause considerable collateral damage if they get out of control.
Method of prevention of oxidative injury to cells
Dec 4, 1985 – US Patent for Method of prevention of oxidative injury to cells (Patent # 4,870,002). ; The United States of America as represented by the Secretary of the Air Force
A process for preventing oxidative injury in which living cells are contacted with a protective amount of 3-amino-tyrosine or a derivative thereof. Also, a process for preventing thermal damage to living cells which comprises contacting the cells with a thermal protectant amount of 3-aminotyrosine or a derivative. Also, a process for protecting living cells from damage caused by ionizing radiation, which comprises contacting the cells with a radioprotectant amount of 3-aminotyrosine or a derivative thereof. Also provided is a process for suppressing inflammatory reactions in animals which comprises administering an anti-inflammatory amount of 3-aminotrosine or a derivative thereof to an animal.
Determinants of the Symptoms and Severity of COVID-19: Russian Roulette?
The first assumptions about COVID were that it would be most severe in the elderly because of compromised immune systems and kill those with underlying chronic conditions, or secondary bacterial infections, mirroring the flu. Another was that either it didn’t infect children or at least those under 9 years of age. Then as infected numbers increased some with no underlying conditions and in their 40’s or less began to get severe disease and even die and children, even less than 9, developed Kawasaki-like syndrome, multi organ inflammation. The illusion and bias of the flu comparison began to evaporate. The question is are these outcomes connected by mechanism and logical progression or are they happenstance or a little of both? The alternate immune pathways and their various combined and graded responses (even independently among their components) and interactions with target tissues make for the great variety of symptoms, severity, and level of viral shedding. The data is growing fast and furious outpacing the interpretation and forming of the big picture. However, I will attempt to summarize and at least give a preliminary interpretation with the proviso that it is subject to modification as new data arises. One of the latest indications that the severity is not uniquely tied to immunosuppression but an inappropriate or misdirected immune response is that in some patients IgG arises prior to IgM. It is usually the other way around for the appearance of these two types of antibody. This could result from cross response of antibody memory cells (B cells) against another CoV or T cell independent B cell direct sole response (T cells can help B cells make antibody, CD4 T cells, or be responsible directly for killing virus infected cells specifically, CD8 T cells). Some patients had little or no antibody response, some who were severely ill had strong IgG antibody responses and little T cell response. Some had weak antibody responses and strong T cell responses of various kinds. Some patients made IgE antibody associated with allergic reactions, even anaphylaxis, the most acute and severe reaction. Various levels of cytokines, pro- inflammatory and anti- inflammatory were observed, connected to severity. Gamma Interferon, which blocks viral replication and stimulates non-specific reactive oxygen and nitrogen species production by white blood cells, had a positive effect on patients but others like TNF alpha, interleukins 1 and 6 had a negative effect. Other interferons (alpha and beta) could have either positive or negative effects, depending on their pro- or anti-inflammatory effects. Treatment with IFN-α2b significantly reduced the duration of detectable virus in the upper respiratory tract and in parallel reduced duration of elevated blood levels for the inflammatory markers IL-6 and C reactive protein (CRP) in one study. CRP is a bio marker for heart disease and may be linked to the exacerbation of heart disease in COVID-19. However, the virus can cap its RNA with methyl groups which helps it prevent detection, inhibition of translation into protein, and destruction associated with interferon effects. In children, interleukin 10, an anti- inflammatory, also had a positive effect, as did broad anti-inflammatory drugs like steroids in adults. Children infected but without symptoms have been shown to carry as much or more virus than infected adults. This could indicate that a robust immune response is not always an effective one. In another study 40% of asymptomatic individuals became seronegative and 12.9% of the symptomatic group became negative for IgG in the early convalescent phase following recovery. In addition, asymptomatic individuals exhibited lower levels of 18 pro- and anti-inflammatory cytokines. These data suggest that asymptomatic individuals had a weaker immune response to SARS-CoV-2 infection. They also shed virus longer up to 19 days. Certain subtypes of IgG antibody were associated with more severe responses while others neutralized virus. Studies suggest there are three types of responders: Immunotype 1, comprised of robust CD4 T cell activation, exhausted CD8 T cells and other reduced peripheral blood T cells, linked with more severe disease whereas Immunotype 2, characterized by more effector CD8 T cells, less CD4 T cell activation and proliferating peripheral blood and memory B cells had less severe disease. Immunotype 3, in which minimal lymphocyte activation response was observed, represents ~20% of COVID-19 patientsh and is important to consider as patients who have failed to mount a robust antiviral T and B cell response. Pathology from an immune response too weak resulted in virus-induced pathology, or an immune response that is too strong led to immunopathology. The data suggest that the immune response of hospitalized COVID-19 patients may fall across a spectrum of immune responses, with distinct immunotypes linked to clinical features, disease severity, and temporal changes in response and pathogenesis. Therefore, the immune response has 3 categories: (1) antiviral (some macrophages and dendritic cells, natural killer cells, cytotoxic T cells, helper and suppressor T cells, antibody making B cells and plasma cells, and gamma interferon; other interferons made by tissue cells: alpha and beta); (2) anti-parasitic granulocyte white blood cells (some special B cells that make IgE, eosinophils, basophils (in tissue mast cells), and all kinds of biochemical mediators: histamine, Prostaglandins, leukotrienes, and kinins); and (3) anti- bacterial and fungal (granulocyte: neutrophils, and monocytes and macrophages). COVID-19 can move through all three types. The worst is type 2 which was meant for worms and other multicellular localized parasites and can be locally severe and if generalized, fatal. The first type can yield TNF (tumor necrosis factor) and gamma interferon which can crank up type 2 and antibody linked to infectious agents which can target 3 and cranks up its non-specific killing. Type 2 is also responsible for allergic reactions up to the most severe acute sometimes fatal anaphylaxis. In my graduate (The Cytotoxic Activity of Peroxidases, 1981) and early USAF research (Type B Cytochromes: Sensors and Switches, CRC Press, 1995), I studied the nonspecific (now called innate) immunity in Types 2 and 3 mediated by oxidative burst and nitric oxide (nitrite) production. These when properly directed kill viruses, bacteria and parasites. When improperly directed they cause acute respiratory distress syndrome (ARDS), shock and death as in COVID and intense swelling, hives, edema, nausea, diarrhea, shock and death in allergic reactions. The other immune types are linked to this type and each other. For example, oxidizing CRP makes it enhance clotting like seen in COVID and leukotrienes enhance oxidative burst of granulocytes and gamma interferon enhances oxidative burst and nitric oxide production but favors the later which is more antimicrobial without whole sale damage to tissue like the oxidative burst (superoxide and peroxide). COVID inhibits gamma interferon production but enhances TNF oxidative burst effects. All this nonspecific damage,”burning down the house to get rid of the rats”, leads to chronic lung and other tissue damage which remains in severe COVID patients who have recovered in spite of and to some extent because of Type 3 macrophage cleanup of the damage and subsequent fibrosis. If this all seems too much then I have succeeded in illustrating treating COVID-19 and its outcome is very complex. In the next post, I will distill this down to a progression with various resolution points.
COVID-19 Clinical Progression related to Lines of Immune Defense: First Line of Defense to the Last Stand
SARS-CoV-2 virus enters the nose or mouth by airborne or hand to face transmission. It finds cells with ACE2 receptors and settles in to replicate. In children, it may multiply with limited effect because of tissue interferon and nonspecific antiviral immunity, suppression of severe non-specific immunity, and finally resolve with local specific (adaptive) immunity. In adults with mild or no symptoms, it may follow a similar course. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7227586/pdf/main.pdf and https://science.sciencemag.org/content/sci/369/6504/718.full.pdf. If the numbers of virions continues to increase unabated, some will descend into the lungs and/or the gastrointestinal tract. In the lungs and GI tract, the virus infects most of the lumen lining cells and some blood vessel lining cells (endothelium), the latter releasing virus into the blood to spread to other organs in the body. The lungs are so widely infected that the normally dark lung fields appear like ground glass or cloudy (bacterial pneumonia is lobular, localized and white density) in chest radiographs. The images resemble non infectious hypersensitivity pneumonitis in humans or “walking pneumonia” caused by tiny, cell wall-less bacteria called mycoplasma. This stage could resolve with oxygen and other support from a balanced T cell and B cell (antibody) immune response. A similar course with nausea and diarrhea occurs in the GI tract but with more likely limited resolution and generating a fecal shedding carrier state. If the virus continues to replicate and spread, the widely spread virus is confronted by the nonspecific, Type-2 anti-parasite-like and/or Type-3 anti- bacterial and fungal immunity, which will kill the virus but cause varying degrees of collateral damage from asthma-like effects to systemic septic-like shock and perhaps death. This last phase will require ventilators, ICU care and other heroics to survive. The last two steps may result in long term or permanent lung, kidney and other internal organ damage. Wear a mask, distance, sanitize and stay safe!
How Gamma Interferon and LPS (inducer of Tumor Necrosis Factor: TNF) Shifts Cells in Culture to Produce Anti-viral Nitric Oxide (indicated by nitrite)
Macrophages are switched from an oxidative burst to less damaging nitric oxide anti-viral production and showing how this sensitized the cells to even respond to weak electromagnetic radiation effects.
Aerosol vs Airborne: What’s in a name? A rose by any other name would smell as sweet!
There have been some very heated discussions over whether SARS-CoV-2 is transmitted by aerosol or not and the equivocation of aerosol with airborne. The most offensive scientific one came from an aerosol scientist who used half an argument and argument from analogy (a no no in argumentation) (https://click.mail.medscape.com/?qs=0c71473589954dc3ec114d76d9de44435cfb8a0efd1e184b71f0af4095b99c4a2a10e1c0a7adb945e7ee568544f8ca712c1a3d36124dd01f) to bad mouth medical experts’conclusions which were based on clinical observations and data (Klompas M, Baker MA, Rhee C. Airborne Transmission of SARS-CoV-2: Theoretical Considerations and Available Evidence. JAMA. Published online July 13, 2020. doi:10.1001/jama.2020.12458). I will address concerns from the viewpoint of a counterproliferation scientist who worked with weapon experts, engineers, aerosol physicists, mathematical modelers, microbiologists, and laboratory and full scale tests of aerosolized biological warfare surrogates to determine how they could spread and their effects be mitigated and method of destruction prevent collateral release and biological contamination. The argument given in the Medscape article is based on mass alone and by analogy extended to pollen. The 1834 argument cited does not take into account electrical charge or convection and buoyancy (fluid displacement based on density, why a feather floats and a dense particle of the same mass falls), and Bernoulli’s principle (Hydrodynamica in 1738), that pressure decreases when the flow speed increases, causing lift of various shapes. Also he doesn’t take into account that as particles approach the nano-size (like a virus) their properties change and mass is no longer a key determinant. Studies have shown that particles stay aloft best between 300 nanometers and 1 micron in size. A minimum particle size of 500 nm is the size for which none of the main mechanisms of deposition are effective. A recent study shows aerodynamic diameters of particles expelled when speaking, singing, or coughing are in bimodal overlapping distributions with peaks at a little over 600 nm and 1.1 microns, approximately, respectively, or 800 nm compositely https://chemrxiv.org/articles/preprint/Comparing_the_Respirable_Aerosol_Concentrations_and_Particle_Size_Distributions_Generated_by_Singing_Speaking_and_Breathing/12789221. For particles larger, deposition increases with increasing particle size because of increased gravitational and inertial transport, while for particles smaller, deposition increases with decreasing particle size because of increased diffusive transport. The deepest penetration of the lungs is with 1-2 micron particles. The 5 micron deposits mostly in the upper respiratory tract and much less in the intermediate branches but receptors for CoV are in these regions. Anything less than 300 nm and more than 1 micron deposit rapidly in the environment. The best aerosols generated artificially or naturally fall between 1-10 microns with the mode at 3.5 and average size around 5 microns. Any biological can be artificially aersolized; even remain biologically active for a given time if packed in the right protein liquid matrix, but some die with drying and others, such aerosols, shrink below the optimal lofting range with evaporation or become sticky to surfaces on increasing charge. Real aerosol transmission rather than just airborne transmission (more general) is seen with Q Fever, Foot and Mouth Disease virus in cattle, and anthrax spores; it is for miles not just feet. The graphic shows an ideal aerosol release model and the picture, the complexity of a surrogate actual release, showing convection, mass and turbulence effects very soon after release. The exponential decay graphic illustrates that distance a significant dose of virus can travel is tied to the initial amount released.

Modeling Aerosol Release
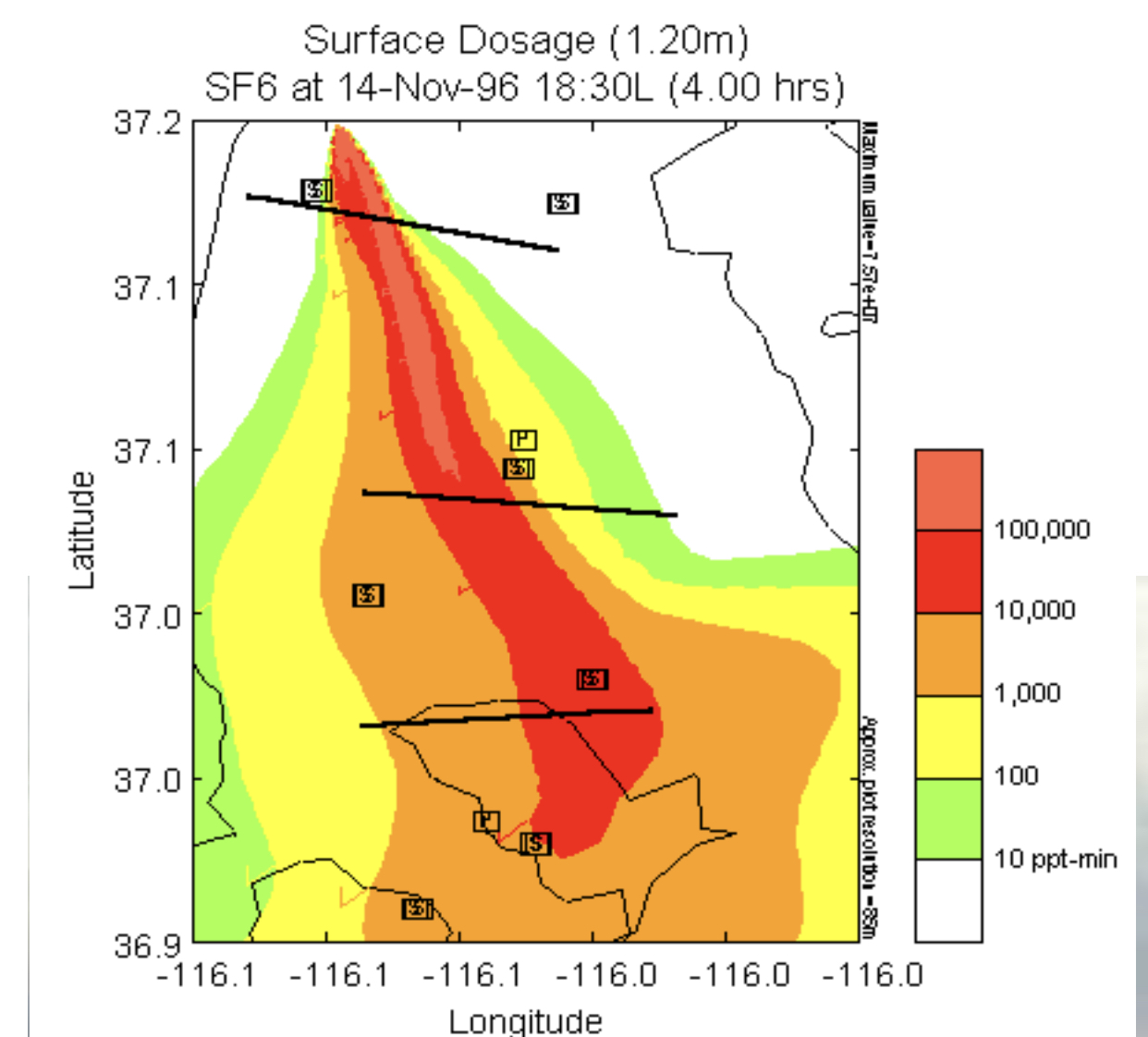
This is a model of the dispersion of an ideal launch of a true aerosol (like anthrax spores where 1 ppm equals 1 microgram or 1 million spores or 100 human lethal doses). One degree of latitude equals 69 miles and one degree of longitude equals 54.6 miles.
Aerosol Release

From this picture one can see a release of particles quickly changes from uniform to a complex distribution of falling ones, rising ones and those that follow chaotic convections and patterns even in still conditions like this one. Why aerosols do not follow simple assumptions:
SARS-CoV-2 Origins 2–To every thing there is a season, and a time to every purpose under heaven
Attribution is very difficult. Recently several conflicting plausible equivocal hypotheses based on genetic evidence on the mechanism of spillover of SARS-2 have been proposed. One says the virus has been in bats 40-70 years prior to its present form and then spread to humans by happenstance, no intervening animals like snakes or pangolins required. The virus just either evolved a gene for human ACE2 receptor binding by mutation and/or the bats had a similar receptor which evolved toward a human compatible form that selected for better binding among viral mutants. A second hypothesis is that the COVID-19 virus was a result of homologous recombination of two very similar viruses infecting the same host cell in an animal or human. This process is very common in coronaviruses. The enzyme, RNA dependent RNA polymerase can shift between 2 template viral RNAs and yield a hybrid third new virus. However, this same enzyme proof reads the new sequences reducing the probability of mutations and mistakes in replication. Examining the genome of SARS-2 shows recombination has happened in the past. One of these possible bat viruses (the other participant is unknown) is SARSr-Ra-BatCoV-RaTG13. The viruses must have very similar RNA sequences for this to happen. The latter has 96.1% genome identity with SARS-CoV-2. Recently another paper has questioned the validity of the methodology for this observation. The problem with RNA is that the host cell can modify it after replication which can lead to different sequences including changing the sequences of subsequent replicates in the future. Also, genetic and computer mathematical analysis indicates that the region of the genome which determines the cell binding appears to not have undergone homologous recombination. So where are we? We need more than genetic analysis to solve this problem. Viruses must be isolated from natural potential sources. In my tenure in the USAF Counterproliferation Team (1989-2011) l had seen this dilemma before in bacteria and viruses. In anthrax, genetic researchers vehemently declared horizontal gene transfer or homologous recombination of its DNA rarely if ever occurred until we found a hemolytic (breaks down red blood cells) and ampicillin resistant anthrax from a biological warfare plant in Iraq. It was not genetically engineered but only exchanged genetic material with a biological insecticide bacteria grown in the vats between anthrax production as a cover for nefarious activity. Later we discovered this could be accomplished with a synthetic nonproteinaceous virus called a nanobe which transferred ampicillin resistance but also inadvertently activated a silent hemolysis gene by homologous recombination. Later an anthrax-like disease was discovered in equatorial Africa in chimpanzees caused by another bacterium carrying anthrax genes, a natural occurrence of the phenomenon. We also discovered that if a gene for the RNA polymerase of VEE {Venezuelan Equine Encephalitis virus) was placed in a retrovirus crippled so it could not infect and reproduce in cells but only express transferred protein genes, a new complete infectious replicating virus appeared. These examples show the flaw in genetic analysis limited by the assumptions of what can happen and how by genetic natural and artificial manipulation.
More on SARS-CoV-2 Animal Nature
Another obvious characteristic of this virus’ infectivity which says it still has strong ties to animal disease is its ability to readily infect minks from humans with probable back infection of humans. Its relative ease of infection of cats and also, but less so, dogs from humans with less probability of back infection to humans is more evidence that the virus still maintains animal infective potential. The disease is not just a zoonosis, it is also a anthroponosis , an infectious disease of humans that can be transmitted naturally to other animals. Another example is tuberculosis (bacterial) transmitted from humans to captive primates and elephants.
