
Global surveillance of infectious disease including pandemics like COVID
Let’s look at vaccine issues and objections; first acknowledging that vaccination has been the greatest medical advance since modern sanitation (including purifying drinking water).
First, modified viruses or cross reactivity of close viral (less pathogenic) relatives were the first vaccines, smallpox and rabies. Smallpox vaccine virus, vaccinia origins are fuzzy, cowpox, extinct horse pox, or weakened smallpox virus? Vaccination started with variolation, an obsolete medical procedure involving the inoculation of a susceptible person with material from the pustules of a smallpox patient to induce a mild form of the disease and hopefully confer immunity. Lady Mary Wortley Montagu, who had witnessed the practice in Turkey, introduced variolation to Britain in the early 18th Century. Benjamin Franklin was also a strong advocate for variolation, even having his own son variolated. Catherine the Great, Empress of Russia, played a significant role in promoting variolation within Russia. Variolation was not without risks. There was a chance of contracting a severe form of smallpox, and some individuals died from the procedure. Variolated individuals could still transmit smallpox to others.
The Jenner vaccine eliminated the former problem but vaccinia could still be transmitted by contact from a vaccinated person to a naive one. On very rare occasion (particularly with an immune suppressed patient) could lead to systemic disease. Edward Jenner postulated that the pus in blisters from sufferers of cowpox (a disease similar to smallpox but much less virulent) protected them from smallpox. On 14 May 1796, Jenner tested his hypothesis by inoculating James Phipps, the eight-year-old son of Jenner’s gardener. He scraped pus from cowpox blisters on the hands of Sarah Nelmes, a milkmaid who had caught cowpox from a cow called Blossom (whose hide now hangs on the wall of the St George’s Medical School library, in Tooting, London).
Even then, people objected to vaccination, like now for exaggerated, often irrational reasons: Some members of the Church believed that disease was sent by God, so the vaccine interfered with God’s will. The vaccine worked by giving people an animal disease. Some people felt that this was not safe and that vaccinated people would grow horns. Although the vaccine has lead to the first and only elimination of an infectious disease in humans (now the niche is being filled by Mpox) we still hear these kind of stange objections. Smallpox was officially declared eradicated on May 8, 1980, by the World Health Organization (WHO). The last known case of natural smallpox infection occurred in Somalia in 1977.
The second elimination of an infectious disease by vaccination was one in cattle, Rinderpest. It was a highly contagious and fatal disease of cattle and other ruminants. It was declared eradicated globally in 2011. This achievement, the second disease to be eradicated after smallpox, was the culmination of a decades-long effort, primarily through the Global Rinderpest Eradication Programme (GREP). The eradication of rinderpest is considered a significant milestone in the field of animal health and a major contribution to global food security and livelihoods.
The production and application of a live whole attenuated vaccine did not always give expected immunity, regardless of its closeness to the original virulent form. Originally, in France, Pasteur and his successors had developed four such anthrax vaccine strains administered in the numerical order of I-IV, with IV being equivalent to wild type fully pathogenic anthrax. At times serum from immune animals was administered in conjunction with the anthrax vaccine. All the strains were administered as vegetative forms and, therefore, were unstable for field use, conferring various levels of immunity and often not halting anthrax outbreaks at all. What was needed was a very stable vaccine that did not require cooling and could endure the conditions of the South African pasture lands as well as the natural disease bacillus.
In 1922, they started using a spore vaccine like one first invented in Australia by amateur bacteriologists John Gunn and John MacGarvie-Smith during the 1890s. It was designed to overcome deterioration during long-term storage and transportation at elevated temperature by exploiting the natural heat-resistant spores. More effective than Pasteur’s vaccine, under severe field conditions, spore vaccines were in widespread use in America, Australia and Japan by the early 1920s. They were first produced at Onderstepoort about the same time.
However, they failed to be protective, demonstrated by failures in the field in 1926 and 1933. An attenuated strain that killed susceptible guinea pigs but not rabbits and provided protection for the latter was required in the laboratory to be considered a vaccine candidate. Heating the cultures to 42°C during culture was considered the way to generate the attenuated vaccine strains. However, this approach is what produced the mixed results experienced in 1926 and 1933.
Max Sterne, an Onderstepoort-trained veterinary scientist and bacteriologist, appointed in 1934 to manage vaccine production, decided to take up the challenge of overcoming these setbacks. Sterne thought previous researchers had missed the potential significance of the link of the virulence of Bacillus anthracis to the ability of the organism to form a “capsule” over the cell wall, which allowed it to evade destruction by phagocytic white blood cells. In the course of propagating a series of these smooth variants, those making capsule, in his attempts to produce immunity, he discovered unencapsulated “rough” mutants. Sterne cited German studies done around 1910, which indicated unencapsulated forms of naturally occurring Bacillus anthracis could sometimes produce immunity. Guinea pigs injected with the unencapsulated, aviru-lent “disassociants” of certain strains were shown to be able to resist very large doses of a highly virulent strain. These results raised the possibility that a completely avirulent vaccine with the stability of previous spore vaccines could solve the problem of safety. A method of consistently producing encapsulated smooth colonies out of which rough mutants could be picked was required.
Sterne theorized that the characteristic roughness of otherwise virulent strains obtained from dead animals might be an adaptation to the culture conditions in the laboratory. The conditions under which Bacillus anthracis normally multiplied, however, were found in the bloodstreams of living animals. Encapsulated smooth cultures might be obtained more easily under conditions which emulated the natural environment for the propagation of the bacteria in the animal body. One of Sterne’s colleagues, the British bacteriologist J. H. Mason, constructed a tube containing a semi-solid medium of horse serum and agar in which the concentration of carbon dioxide could be controlled.
Using this innovation, Sterne found he could easily grow encapsulated smooth variants which regularly produced visible colonies of mutants of rough unencapsulated bacilli. These unencapsulated variants all turned out to be avirulent when injected into guinea pigs and some gave a good degree of protection against the injection of virulent cultures.
He eventually chose an unencapsulated variant of a strain isolated from a severe outbreak, designated 34F2. To produce the vaccine, bacilli were picked from the rough colony, allowed to sporulate, and then freeze-dried. When vaccine was needed, the manufacturer germinated the spores and propagated them in large quantities on solid agar. These cultures were then allowed to sporulate in oxygen and washed off into saline at a standard concentration for division into individual doses.
The avirulent nature of the new vaccine was very important because it now im-munized, rather than killed guinea pigs,
making them useful for testing the level of protection produced by the vaccine.
Furthermore, these results for the guinea pig were predictive for large animals, so there was no longer the need for expensive large-scale testing on sheep. Initially a small number of animals were injected in the field to check that the vaccine produced no severe reactions. Vaccine derived from strain 34F2 was used for all animals (this strain still killed mice), but smaller doses were used for horses and goats. The “avirulent” vaccine was first released for field trials in 1936 and used on a large scale beginning in 1938. This vaccine is still used today globally for large animals.
For anthrax, like many modern vaccines such as DPT for other bacterial diseases, the antigen the vaccine is actually effective against is the toxin rather than the bacterium itself, and toxoids (“detoxified” toxins must be included in the vaccine such as for diphtheria and tetanus and, in part, pertussis) are included in the vaccines.
The pXO1 and pXO2 plasmids in Bacillus anthracis, which are crucial for its virulence, were discovered in the late 1980s and early 1990s. Specifically, pXO1, which carries the genes for anthrax toxins, was identified by Makino et al. in 1989. It is still in the Sterne vaccine strain. The pXO2 plasmid, which encodes the capsule that protects the bacteria from the host’s immune system, was identified by Reif et al. in 1994 was eliminated from the Sterne strain making reversion to a pathogenic one impossible. PA is the key targetted antigen to block both anthrax toxins and confer protective immunity by the vaccine.
The live virus vaccine objections have had some merit due to mutation reversion in attenuated oral polio vaccine (now replaced by killed vaccine, but with still some persistence of the live oral less pathogenic strain, due to prior use, in certain populations in other countries, spread through contaminated water and poor sanitation). Other live vaccines have been removed because of reversion to pathogenic forms, or on rare occasion, failure to provide sufficient protection from wild type disease. Examples being modified live rabies vaccine which gave strong protection in dogs but could revert to cause rabies in cats and primates, Venezuelan Equine Encephalitis live vaccine (TC83) that could revert, cause fever, or fail to protect because the attenuated form had so few genetic changes and the very simple genome of the pathogenic form, Strain 19 Brucella vaccine in cattle because it persisted in cattle as a low-grade infection, causing false positives on brucella tests, and because it caused brucellosis in humans (accidentally self-inoculated). Strain 19 was replaced by RB51 Brucella vaccine to avoid the false positives and human disease. There have been less human infections. but still a few.
The Johnson & Johnson Adenovirus vaccine is a non-replicating COVID spike-gene-containing virus that induces synthesis of the COVID spike protein from copy DNA inserted in its genome. Other viruses used to make desired vaccine proteins from nucleic acid templates include canary pox virus (in vaccines for canine distemper virus, feline leukemia virus, or West Nile virus). and modified retroviruses (vaccine platform specifically aimed at inducing immune responses against Hepatitis C Virus (HCV) antigens displayed by recombinant retrovirus-based virus-like particles (VLPs) made of Gag protein of murine leukemia virus). Naked DNA vaccines delivered by nanoparticles or electroporation have also been made but are less popular. DNA vaccines have been approved for use in certain animal diseases, such as West Nile Virus in horses and melanoma in dogs. They are also being developed for Human Immunodeficiency Virus (HIV) and Cancer: Research is ongoing to explore the potential of DNA vaccines for these diseases. The DNA must be transcribed into messenger RNA (mRNA) then translated into proteins to be immunogenic. This is true for all live virus vaccines and carrier virus vaccines,
DNA and mRNA vaccines must have the protein antigens expressed from nucleic acid templates to be immunogenic and protect against infectious diseases. Their advantage compared to attenuated or carrier viruses is they have no proteins, except those expressed after administration. Like live vaccines they do not deliver a finite amount of antigen or just protein as killed vaccines do. The nucleic acid vaccines (DNA or mRNA) can only deliver immunogens they are programmed for. They have finite life times in host cells and mRNA is even more fragile than DNA because of the arsenal of enzymes in cells to destroy RNA even with modifications to delay them. mRNA do not need to travel to the nucleus, like DNA, to be translated into the protein antigens.
Another concern is preservatives and adjuvants. Preservatives such as antibiotics and thimerosal (thio ethyl mercury) are necessary because the viruses for vaccines are grown in cell culture or embryonated chicken eggs (standard influenza vaccines which may become contaminated with bacteria that can grow alongside the viruses in production or after bottling and produce products such as endotoxin that are harmful even at low concentrations.)
The claims of toxicity are because of confusing different compounds of mercury, like methyl mercury which is more toxic than ethyl mercury. Mercuric chloride has been used in medicine as an antiseptic and syphilis treatment, its toxicity and corrosive nature led to its discontinuation in modern medical practice. All compounds of mercury are not equivalent in toxicity.

Adjuvants have been blamed for a variety of adverse effects of vaccination through induction of chronic inflammation (linked to cancer in humans in general, other mammals, and, particularly, in cats through injection site fibrosarcomas). However, they are necessary to achieve robust immune responses to vaccines by triggering the non-specific innate response which then triggers a specific immune response that supersedes innate responses and suppresses the former when adequate specific immunity is achieved. Among the most commonly used ones are:
Aluminum Salts (Alum):
These are the most widely used adjuvants in human vaccines, found in
vaccines for hepatitis A, hepatitis B, and others. They are known to promote
a Th2-biased immune response, which is important for antibody production.
Oil-in-water emulsions:
MF59 and AS03 are examples, composed of squalene, polysorbate 80, and other components. They are used in influenza vaccines and other vaccines.
These emulsions can prolong antigen exposure and enhance antigen
presentation.
Saponins:
These natural compounds, found in the bark of the Quillaja saponaria tree,
are used in adjuvants like Matrix-M™, which is used in the R21/Matrix-M
malaria vaccine. Saponins stimulate both humoral and cellular immune
responses.
TLR Agonists:
These adjuvants mimic pathogen-associated molecular patterns (PAMPs)
and activate Toll-like receptors (TLRs), triggering immune responses. CpG
1018, a TLR9 agonist, is used in some vaccines.
In humans, up until the 1960’s, no virus was thought to cause cancer. Epstein-Barr virus (EBV) was first discovered in 1964, in Burkitt lymphoma cells. Researchers Anthony Epstein, Yvonne Barr, and Burt Achong identified the virus in a cell line derived from a patient with Burkitt lymphoma. This discovery marked the first time a human virus was shown to be associated with cancer. However, it does not always cause cancer, lymphoma appearing predominantly in children, causing “Kissing Fever”, mononucleosis in youths and adults. A breakthrough vaccine against a virus that causes cancer in humans was developed in 2006. The Human Papillomavirus (HPV) vaccine is a vaccine that protects against infection by certain types of HPV and protects against several types of HPV that can cause cervical, vaginal, vulvar, penile, anal, and oropharyngeal cancers. It also prevents genital warts caused by certain HPV types. The CDC recommends routine vaccination for adolescents starting at age 9-12, and it can be given up to age 26 for those not previously vaccinated or with a weakened immune system. The HPV vaccine has been shown to significantly reduce HPV infections, genital warts, and precancerous cervical changes. ACOG recommends it as an important tool for cancer prevention, and it is recommended that healthcare providers increase vaccination rates.
Lipid nanopa!icles:
These are used extensively in mRNA vaccines to deliver the mRNA and also
have an adjuvant effect, enhancing the immune response.
Amongst these, aluminum has been attacked the most recently by those who oppose vaccination, especially of children but this accusation has not stood up to the data and scientific analysis.
The most notorious adjuvant historically is Freund’s Adjuvant, only used in research in mice and rats and other research animals to experimentally induce a strong immune response. Freund’s adjuvant is a water-in-oil emulsion that helps prolong the release
of antigens, leading to a stronger and longer-lasting immune
response. It is named after Jules T. Freund, who developed it in the 1940s. Complete Freund’s Adjuvant includes heat-killed mycobacteria (like Mycobacterium tuberculosis) in addition to the oil emulsion. Freund’s adjuvants are not for human or veterinary use. CFA can cause significant side effects, including infammation, pain, and granulomas.
The most notorious example of vaccine adjuvant associated reactions is in cats, injection site fibrosarcomas. Feline injection-site sarcoma specifically denotes a type of cancer, often linked to injections (FISS). While adjuvants are crucial for vaccine efficacy, they can also trigger inflammation at injection sites, and in some predisposed cats, this inflammation may contribute to the development of FISS. The link is tenuous as vaccine causative because of the often long delay in the cancer development (up to years). Also, chronic inflammation is a non-specific promoter and weak initiator of the appropriate genetic changes of proto-oncogenes (necessary for normal growth and development of tissues) possibly through inflammatory oxygen free radical or nitric oxide/nitrite damage to DNA causing initiating mutations. The condition is rare and specifically results in sarcomas (specifically, fibrosarcomas). This specificity is unique for such a non-specific cause. This specificity could result from the site of injection chronic inflammation or something more hidden.
The fibrosarcomas are found in young cats more often than non-injection site fibrosarcomas (in cats mostly 11 years or older). The FISS are more aggressive and likely to fatally metastasize, and there seem to be predisposing factors. These characteristics suggest a viral association, although the common ones such as feline leukemia/lymphoma virus and the defective feline fibrosarcoma virus are not consistently present. The search for other viral causes or integrated components have not been exhaustively examined. Cats have endogenous retroviruses that can be expressed or defective integrated in the genomic DNA. An uncharacterized class of endogenous gammaretroviruses, termed ERV-DCs are present and hereditary in the domestic cat genome. Infectious gammaretrovirus is capable of infecting a broad range of cells from various species. Studies indicate that ERV-DC10 entered the genome of domestic cats in the recent past and appeared to translocate to or reintegrate at a distinct locus as infectious ERV-DC18. ERV-DC-like sequences were found in primate and rodent genomes, suggesting that these ERVs, and recombinant viruses such as RD-114 and BaEV (RD-114 is a feline ERV, while BaEV is a baboon ERV ) originated from an ancestor of ERV-DC. They found that a novel recombinant virus, feline leukemia virus subgroup D (FeLV-D), was generated by ERV-DC envelope gene transduction into feline leukemia virus in domestic cats. These results indicate that ERV-DCs behave as donors and/or acceptors in the generation of infectious, recombinant viruses. A precedent exists for defective viral recombination generating fibrosarcomas. Feline sarcoma virus (FeSV) is a type of retrovirus that causes tumors in cats, primarily fibrosarcomas (tumors of connective tissue). It’s a recombinant virus, meaning it’s formed by combining genetic material from Feline Leukemia Virus (FeLV) and the cat’s own cellular genes (specifically oncogenes). FeSV is replication-defective, requiring the presence of a helper FeLV to replicate.
Although vaccines or their adjuvants may be accused of causing cancer, at least in cats and much less so in dogs, they have a place in actually preventing cancer, such as for Feline Leukemia in cats and Marek’s Disease in chickens. Marek’s disease (MD) is a highly contagious viral disease in poultry, and vaccination is a key preventative measure. The Marek’s disease vaccine, typically a live virus, is administered to day-old chicks to help protect them from developing the disease and its associated tumors. Vaccinated birds can still become infected with MDV and potentially transmit it to unvaccinated birds, although the vaccine reduces the severity of the disease.
The final objection, beyond non-specific inflammatory reactions to vaccines, is allergic reaction to vaccines. This is wholly determined by the host. All vaccines have the potential to cause allergic, largely histamine mediated, acute reactions, swelling of the face, diarrhea, nausea, and hives (urticaria). However, any protein and some non-proteins can cause this, examples, peanut and penicillin, respectively. These on very rare occasions can be so severe that accidental aerosols from use in a confined area or drawing up the penicillin can cause even life threatening reactions. These are usually very rapid within 20 minutes up to 2 hours. Delayed reactions may arise from immune cellullsr responses,other than IgE and mast cell responses, which last longer than two hours to days. Allergic or hypersensitivity or autoimmune reactions to vaccines are usually the result of irrelevant antigens (those not responsible for the neutralization of the pathogens or prevention of disease) such as egg proteins in influenza vaccines because the viruses are grown in embryonated chicken eggs.
An autoimmune reaction often associated with vaccination is Guillain-Barré syndrome (GBS), an autoimmune disorder where the body’s immune system mistakenly attacks the peripheral nerves, leading to nerve damage and muscle weakness. However, the most common trigger for GBS is infection with Campylobacter jejuni, a bacterium that causes gastroenteritis, or infection of the digestive tract, the most common cause of food borne illness.
The first rabies vaccine was made from virus grown in rabbits and made from their spinal cords, leading to allergies and autoimmunity because of the presence of the rabbit neuronal proteins in the vaccine. This was replaced with vaccine produced in embryonated duck eggs with egg proteins on occasion causing allergic reactions, and finally from human cell cultured virus, which has the lowest probability of causing allergic reactions in humans. These irrelevant proteins may be introduced during the production of the vaccine.
When discovered, modern vaccine producers make every effort to remove these potentially allergenic materials. A classic example of this is in historical leptospirosis vaccines (more correctly called bacterins, killed pathogenic bacterial preparations) used in veterinary medicine. The media to grow leptospiras usually contains rabbit serum or bovine serum albumin that can trigger allergic reactions. Newer growth media or a protein extraction method are used in modern leptospirosis vaccines to reduce the potential for a reaction or make it no more frequent than with other canine vaccines. Rabbit serum provides essential nutrients and factors that support the growth of Leptospira, including native hemoglobin and other growth-promoting substances.
The concentration of rabbit serum in Leptospira media can vary between 3% and 10%.
Common media:
EMJH medium, a widely used medium for Leptospira, is often supplemented with rabbit serum.
Other media:
Other media, like Fletcher’s medium, also utilize rabbit serum for Leptospira cultivation.
Variations:
Some pathogenic strains may require specific supplements, like Ellis’s T80/40/LH medium, which includes polysorbate 40, lactalbumin hydrolysate, and superoxide dismutase along with rabbit serum.
Protein-Free Options:
Protein-free and low-protein media have also been developed, such as one based on charcoal-detoxified Tween and another supplemented with 0.1% bovine serum albumin.
Finally, in respect to COVID vaccines triggering autoimmunity compared to the infection itself:
Coronaviruses in general and SARS-CoV-2 in particular are associated with T17 pathway activation which plays a role in autoimmunity. I suspect repeated SARS-CoV-2 infections would more likely trigger autoimmunity (IgG4) than mere vaccination. Type T17 immunity is a specialized immune response crucial for defending against certain extracellular bacteria and fungi, particularly those that cause mucosal tissue damage, and intestinal parasites. It’s a distinct arm of the immune system, mediated by T helper 17 (Th17) cells and group 3 innate lymphoid cells (ILC3s), and characterized by the production of the cytokine IL-17A. This type of immunity is important for maintaining mucosal homeostasis and can be involved in both protective and inflammatory responses. Dysregulation of type 17 responses can contribute to chronic inflammatory disorders, such as inflammatory bowel disease (IBD) and other autoimmune diseases.
All modern vaccine producers have carefully considered all these potential problems, and the best of biomedical science has worked hard to reduce them to insignificance so vaccines can continue to save millions of lives from suffering and death.
Selected References
Verstraeten T, Davis RL, DeStefano F, Lieu TA, Rhodes PH, Black SB, Shinefield H, Chen RT; Vaccine Safety Datalink Team. Safety of thimerosal-containing vaccines: a two-phased study of computerized health maintenance organization databases. Pediatrics. 2003 Nov;112(5):1039-48. Erratum in: Pediatrics. 2004 Jan;113(1):184. PMID: 14595043.
Kinney RM, Chang GJ, Tsuchiya KR, Sneider JM, Roehrig JT, Woodward TM, Trent DW. Attenuation of Venezuelan equine encephalitis virus strain TC-83 is encoded by the 5′-noncoding region and the E2 envelope glycoprotein. J Virol. 1993 Mar;67(3):1269-77. doi: 10.1128/JVI.67.3.1269-1277.1993. PMID: 7679745; PMCID: PMC237493.
Woodward KN. Origins of injection-site sarcomas in cats: the possible role of chronic inflammation-a review. ISRN Vet Sci. 2011 Apr 12;2011:210982. doi: 10.5402/2011/210982. PMID: 23738095; PMCID: PMC3658838.
Zajc AL, Harper A, Benoit J, Mason S. Non-injection-site soft tissue sarcoma in cats: outcome following adjuvant radiotherapy. J Feline Med Surg. 2022 Aug;24(8):e183-e193. doi: 10.1177/1098612X221098961. Epub 2022 May 31. PMID: 35639367; PMCID: PMC10812266.
Anai Y, Ochi H, Watanabe S, Nakagawa S, Kawamura M, Gojobori T, Nishigaki K. Infectious endogenous retroviruses in cats and emergence of recombinant viruses. J Virol. 2012 Aug;86(16):8634-44. doi: 10.1128/JVI.00280-12. Epub 2012 Jun 6. PMID: 22674983; PMCID: PMC3421742.
Esau D. Viral Causes of Lymphoma: The History of Epstein-Barr Virus and Human T-Lymphotropic Virus 1. Virology (Auckl). 2017 Sep 25;8:1178122X17731772. doi: 10.1177/1178122X17731772. PMID: 28983187; PMCID: PMC5621661.
Leonard RA, Spurrier MA, Skavicus S, Luo Z, Heaton BE, Spreng RL, Hong J, Yuan F, Heaton NS. Development of DNA and mRNA-LNP vaccines against an H5N1 clade 2.3.4.4b influenza virus. J Virol. 2025 Jul 16:e0079525. doi: 10.1128/jvi.00795-25. Epub ahead of print. PMID: 40667976.
This kind of technology is needed more than ever to counter bioterrorism/biowarfare which has become an even more imminent threat now that Iran is motivated to respond with asymmetric warfare and found new support to respond to US bound to the Israeli war, by giving reason for uncertainty in any alliances in the Middle East beyond Israel. Bioterrorism is even more likely now with dismantling means to rapidly respond to infectious disease and blinding our intelligence gathering by alienating our allies. US cannot be an island unto itself. It needs global cooperation to survive.The following is given in more detail, with background references, in Bionanotechnology: Radio Controlled Antimicrobial and Genetic Vectors (Springer-Nature, 2024) and The Black Dragon Trilogy (Amazon eBooks, 2018):
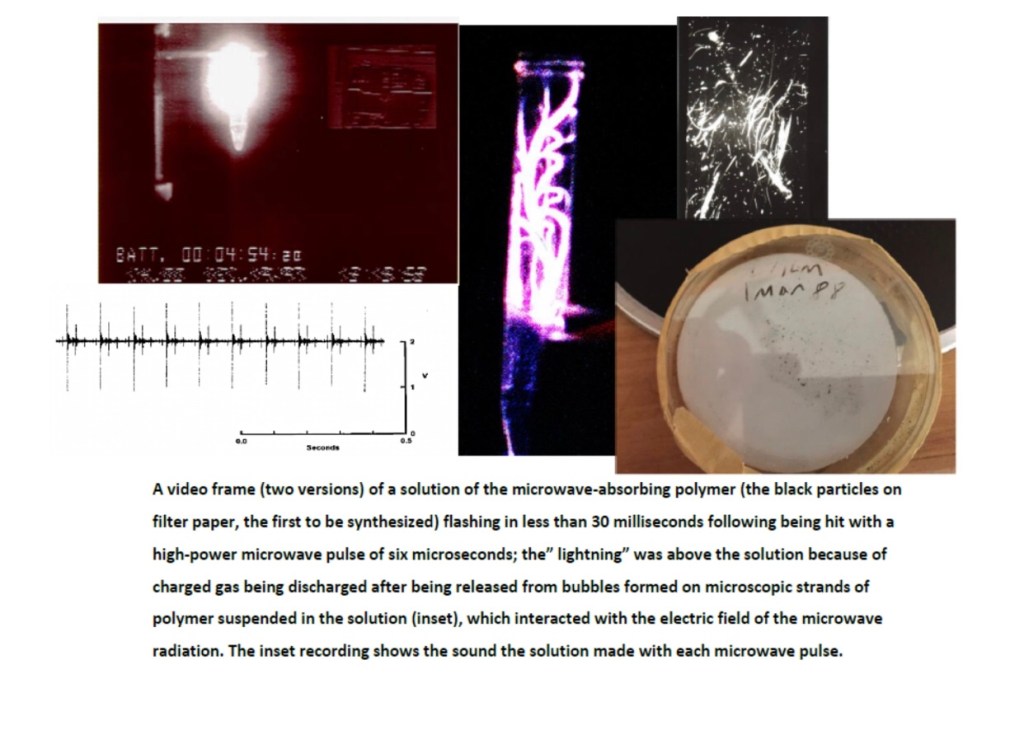
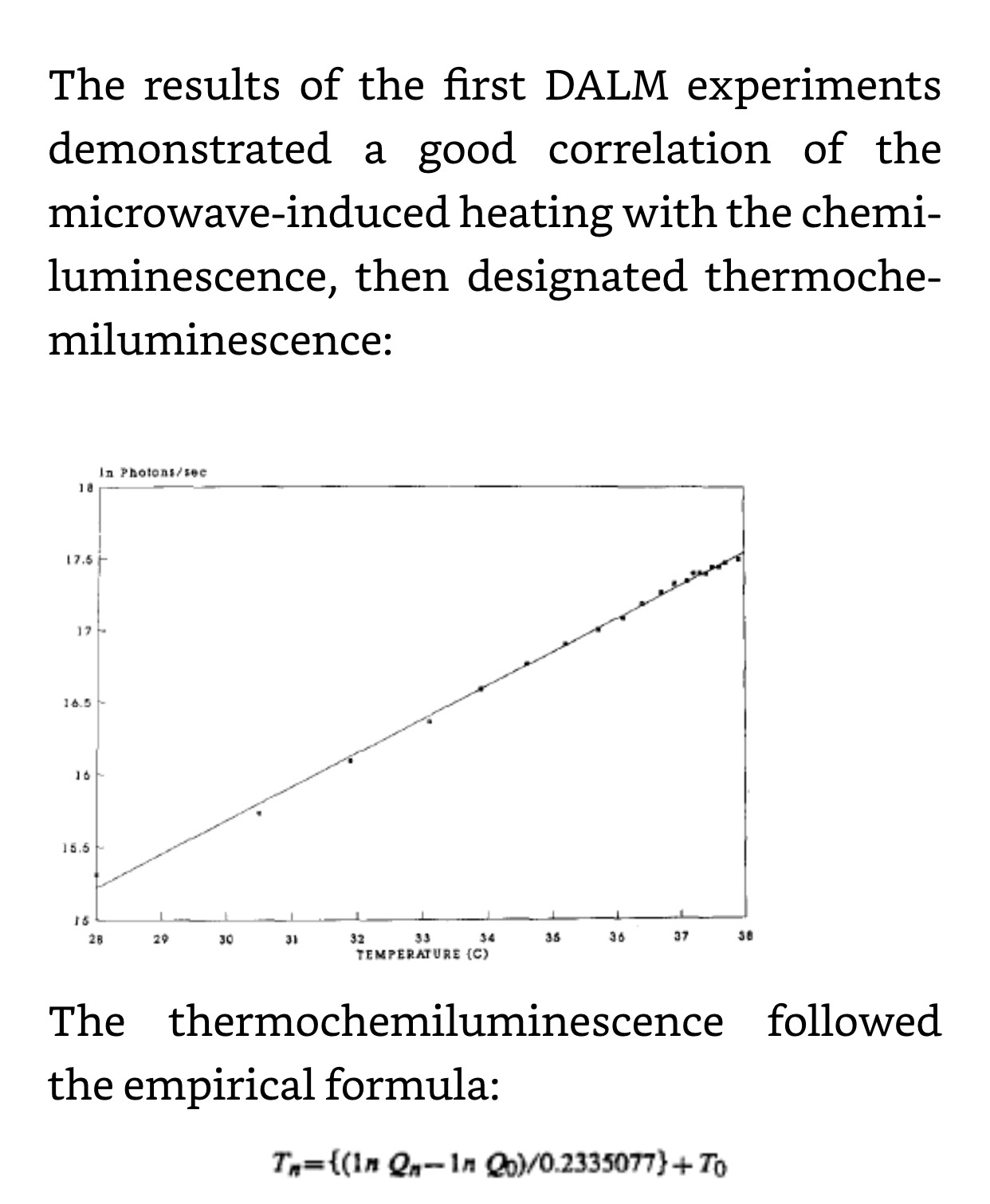
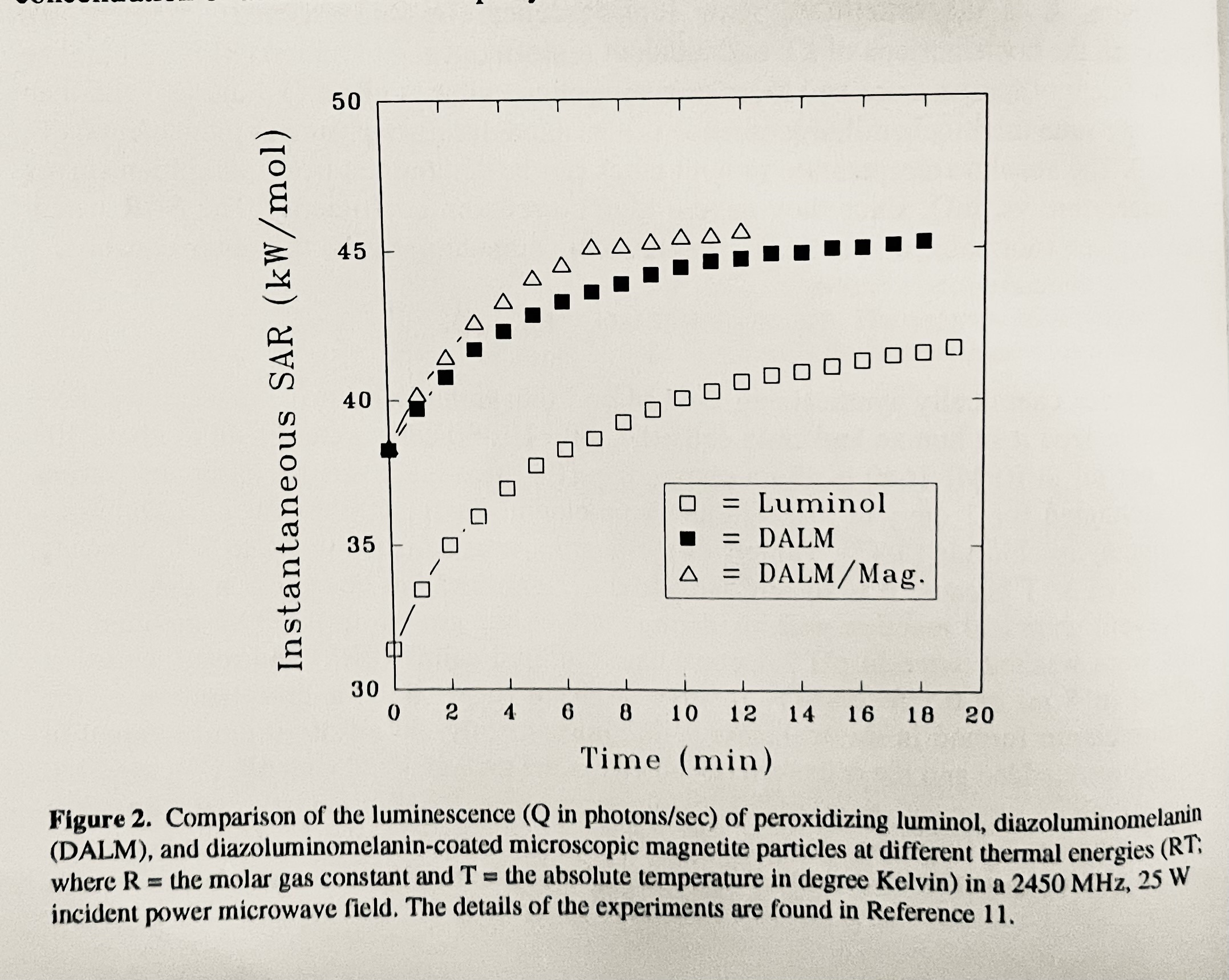
The classic thermochemiluminescent response of oxidizing DALM to microwave heating.



This technology has now been shelved but is fully described in Bionanotechnology: Radio Controlled Antimicrobial and Genetic Vectors, Springer-Nature, 2024.
Available now! Paperback coming out soon.This book is for scientists, engineers, students, and all others who wish to pursue the interdisciplinary collaborative approach to solving major technical problems leading to highly significant products. It represents the completion of my 43-year mission (as part of the USAF biosurveillance and Counterproliferation Team of AFRL and as a DoD DTRA contractor consultant thereafter) to deliver technology to detect, collect, identify and neutralize, semi-autonomously, especially dangerous pathogens and biotoxins, as close to the source in non-permissive territory as possible, released into the environment either nefariously or naturally. This work presents a nanomaterial that is activated to kill infectious agents with nonionizing electromagnetic radiation. The bionanotechnology is shared within this book to counter nefarious use and ensure beneficial applications, including a new approach to overcome antimicrobial resistance and mutation that escapes vaccine efficacy. Hopefully, this book will make the biotech and nanotechnology industries aware of the great potential of the radio and microwave frequency controlled bionanotechnology described herein before it is forgotten only to be rediscovered. Furthermore, it provides a plausible explanation for the Havana Syndrome.
This book represents the completion of my 43-year mission (as part of the USAF biosurveillance and Counterproliferation Team and as a DoD contractor consultant thereafter) to deliver technology to detect, collect, identify and neutralize, semi-autonomously, especially dangerous pathogens and biotoxins, as close to the source in non-permissive territory as possible, released into the environment either nefariously or naturally. This work presents a nanomaterial that is activated to kill infectious agents with nonionizing electromagnetic radiation. The bionanotechnology is shared within this book to counter nefarious use and ensure beneficial applications, including a new approach to overcome antimicrobial resistance and mutation that escapes vaccine efficacy. Hopefully, this book will wake up the biotech and nanotechnology industries to the great utility of the radio and microwave frequency controlled bionanotechnology described herein. Furthermore, it provides a plausible explanation for the Havana Syndrome.
Bionanotechnology: Radio Controlled Antimicrobial and Genetic Vectors
https://a.co/d/8ntHvmy
Post script: Recently, a privately, modestly funded R&D project ,The J&R Project, has demonstrated a formulation of the material that can kill biofilm in water systems over months with environmentally available reactants and ambient energy sources. The composition is autonomously maintained.
Perhaps this is my last recourse. The warning has been ignored for far too long (“forced retirement” assured that). Perhaps it is already too late. Let’s hope not.
“Yesterday is gone. Tomorrow has not yet come. We have only today. Let us begin.”–Mother Teresa of Calcutt
This is my agony and ecstasy. This post provides the focus and end of my research, perhaps providing clarity to why I am now in the position I am in, excluded, “forgotten”, and out in the cold.
“When one has nothing more to lose, the heart is inaccessible to fear.”–St. Thodore Guri
The following defied the paradigm of classical microwave “hearing” and brought in the paradox of the quantum world.
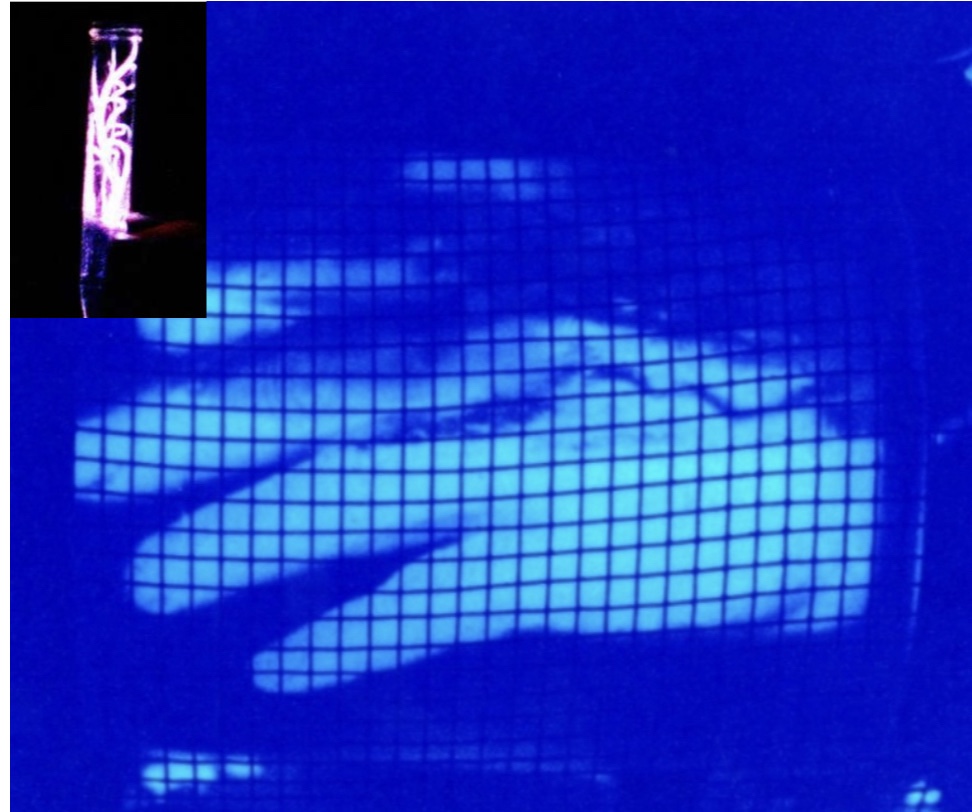
I suppose it was worth suppressing in spite of all the documentation (government reports, peer-reviewed publications, patents, GMO cells, bacterial, animal, and human, deposited at ATCC), independent verification, photographs and hours of video. “ I’ve seen (and heard) things you people wouldn’t believe—all those moments lost in time like tears in the rain.”
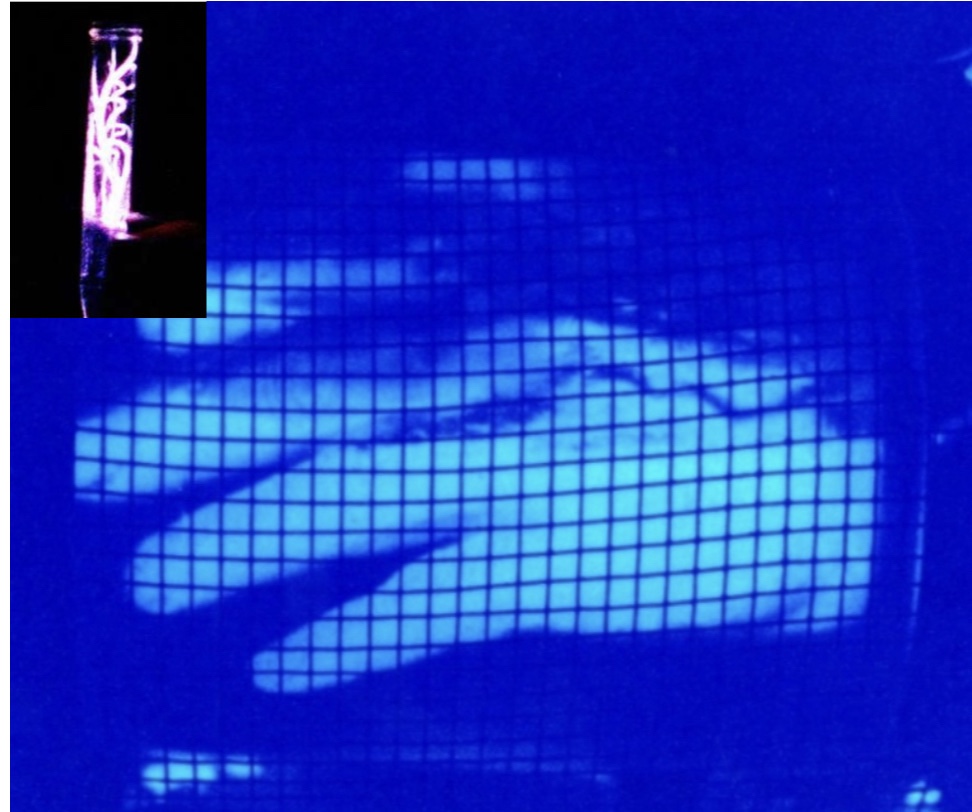
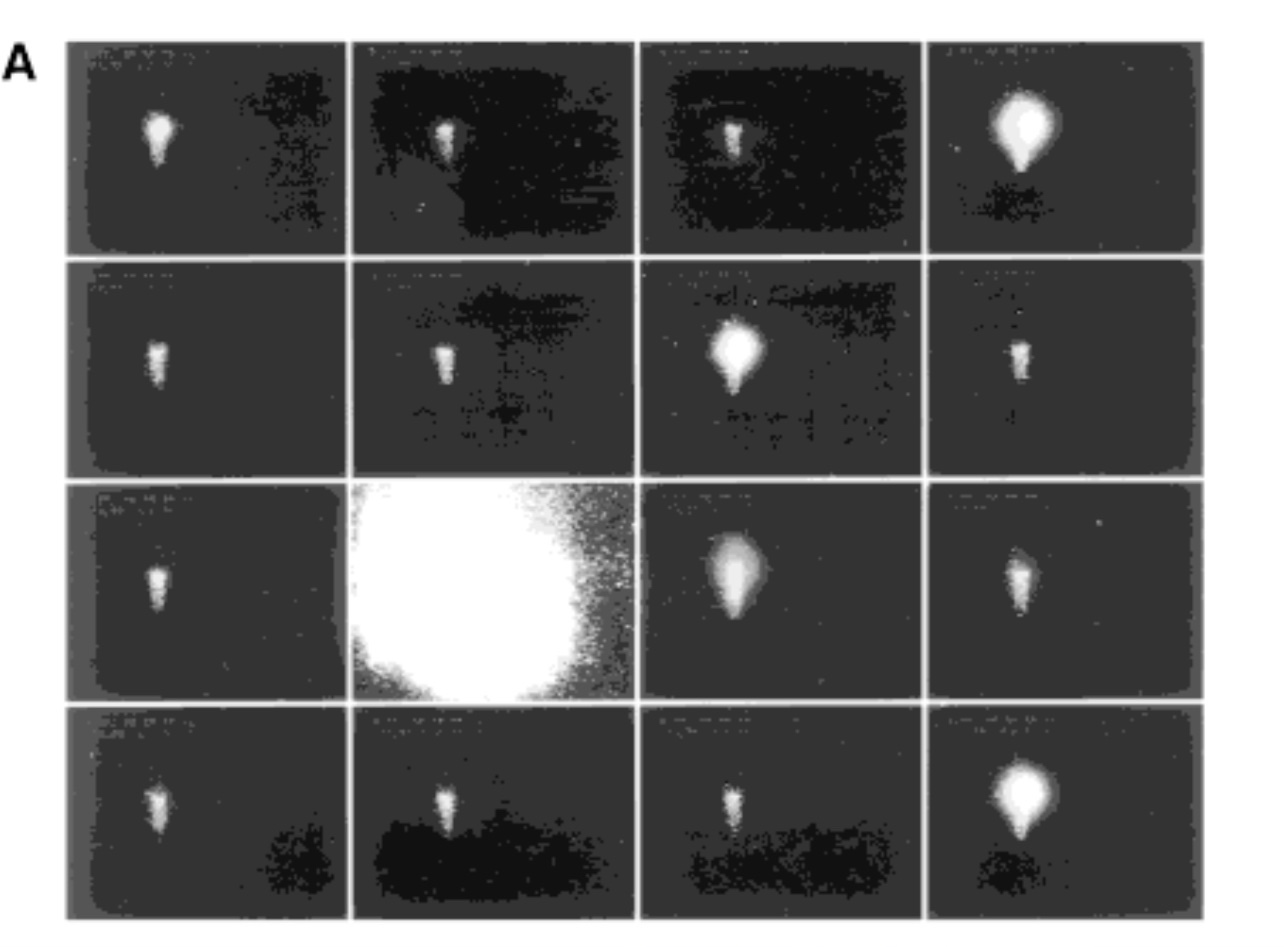
The above is a short video of sound and light generated by microwave pulsed radiation, but at a level of energy focusing that far exceeds that expected by direct thermoacoustic effects responsible for microwave hearing: can also be seen at https://youtu.be/8gQsXfQwkq0. Perhaps this should not be just called “lightning in a bottle” but “Sun in a bubble”?
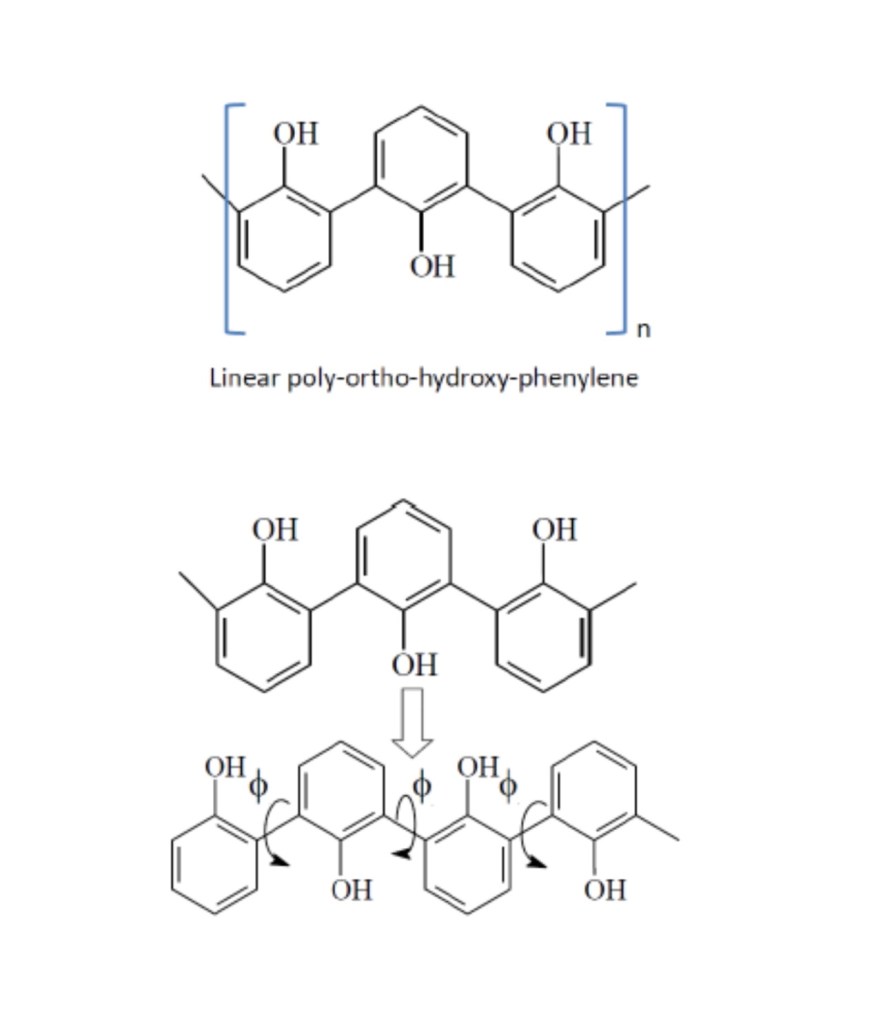
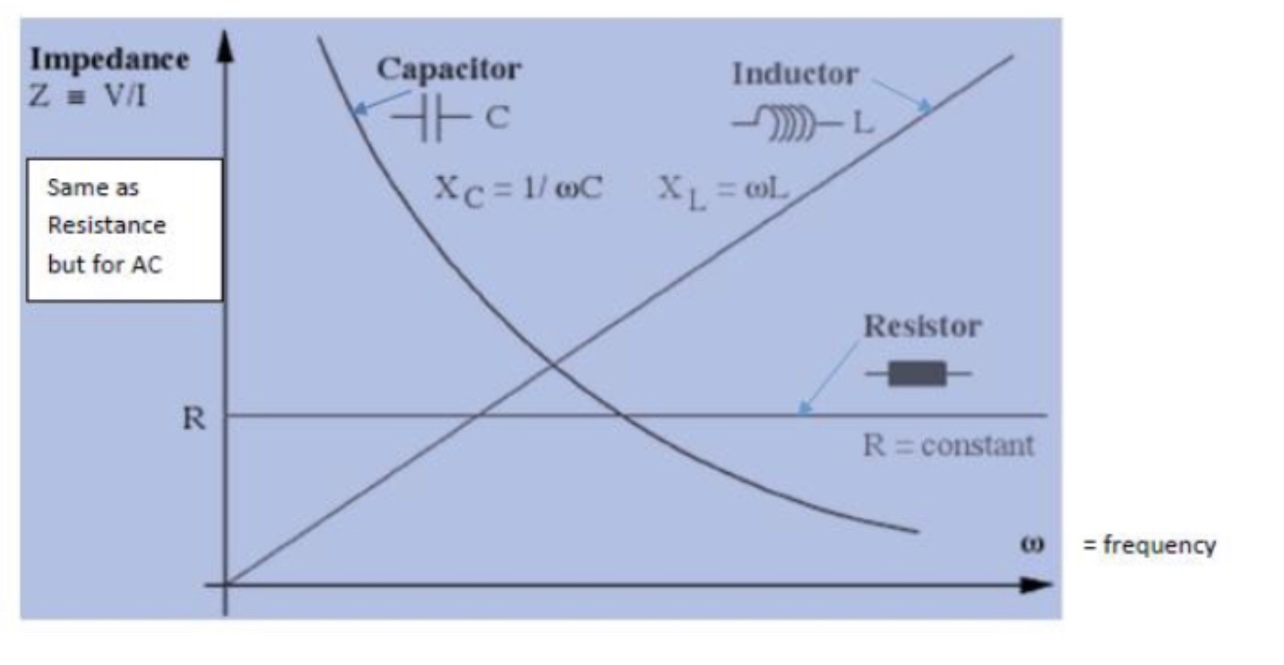
To understand this phenomenon and why it is perceived as a dual use, nefarious, threat, I will summarize 30 years of research that illustrates the problems we intended to solve and solutions that emerged and how needs drove the applications, The first major problem was taking radiofrequency and microwave radiation (RFR and MWR) and focusing this dispersive energy down to the molecular or at least nano level. Classically, it is best absorbed in objects with dimensions from 1/4 to 1/2 the wavelength of the specific frequency of radiation. Also, as the wavelengths shorten (frequencies get higher) to gain absorption of energy into smaller and smaller objects, the penetration of the radiation becomes shallower and shallower. Impedance differences in most materials of this radiation leads (transfer of power from impedance mismatch of source to object) to heating and loss of movement of the electric field through the exposed objects.
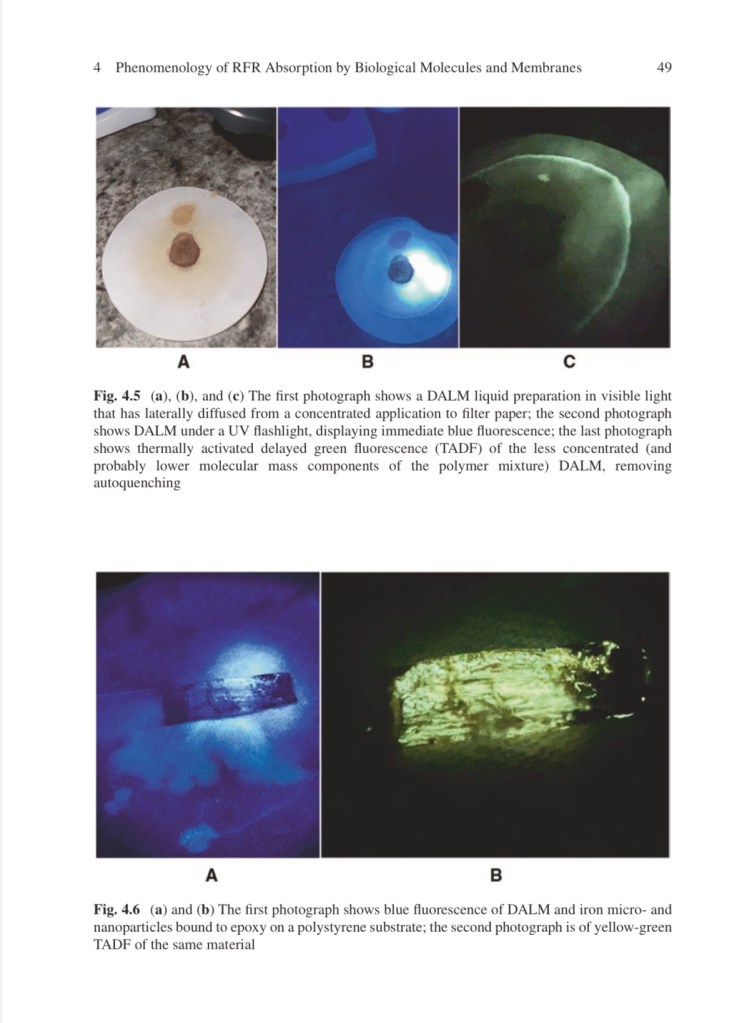
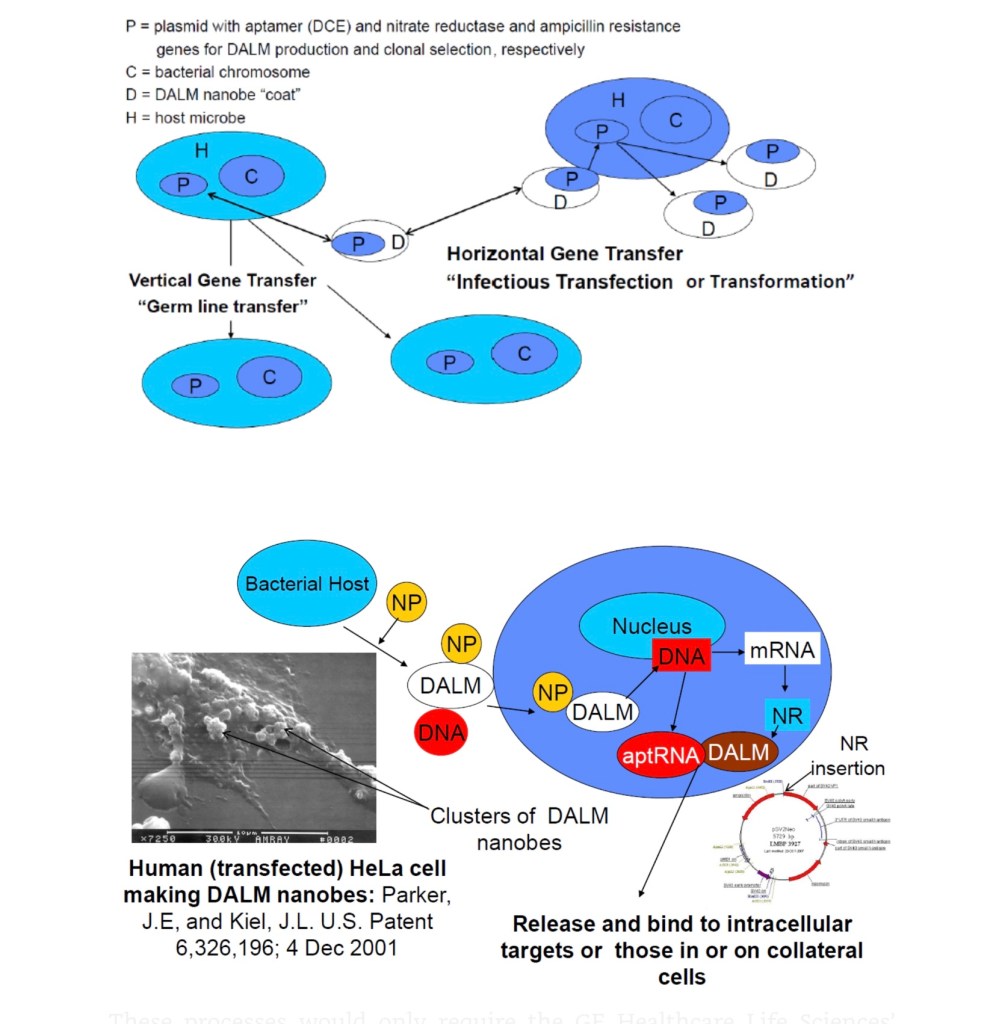
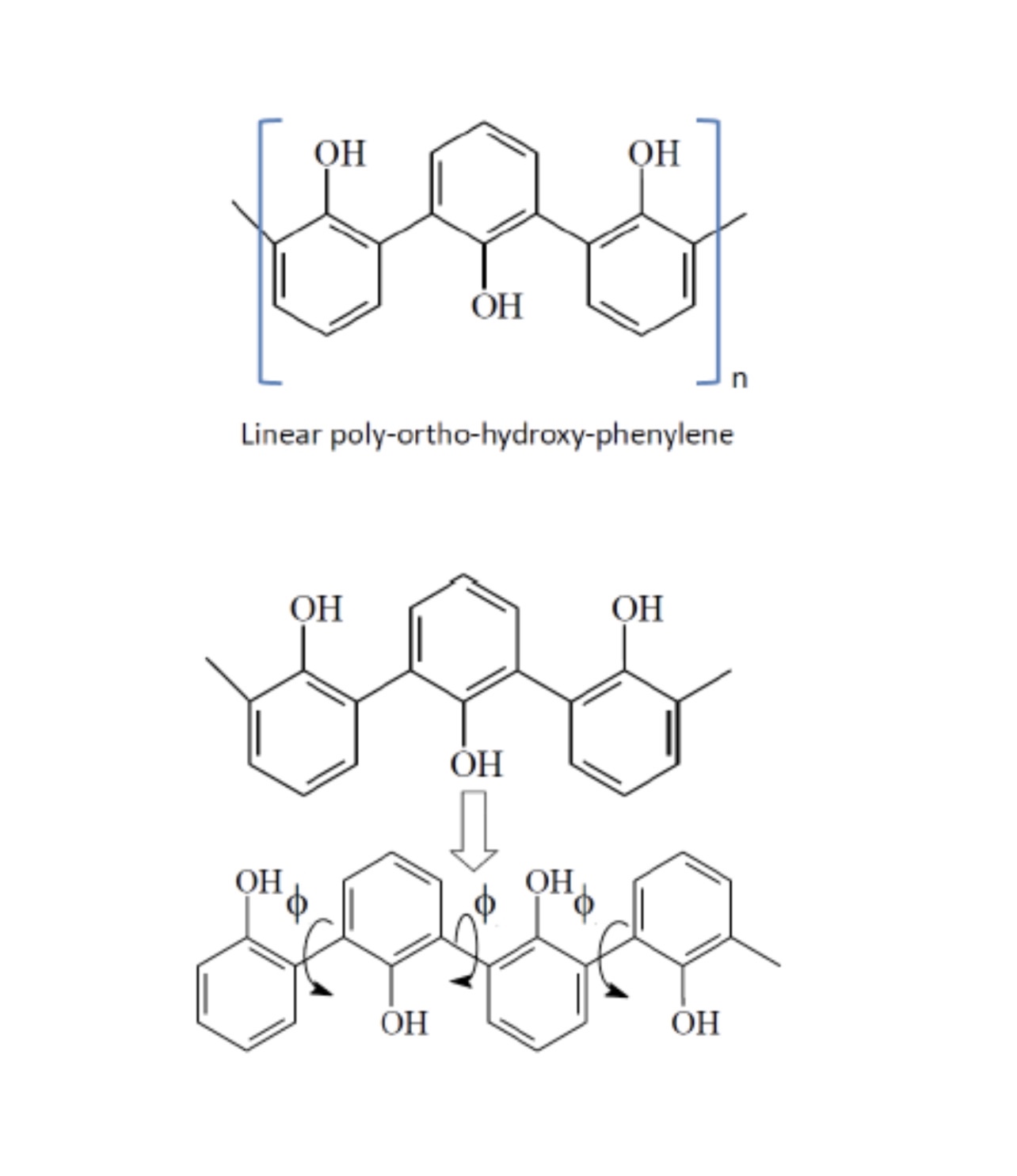
DALM: diazoluminomelanin, poly-ortho-hydroxy-phenylene:


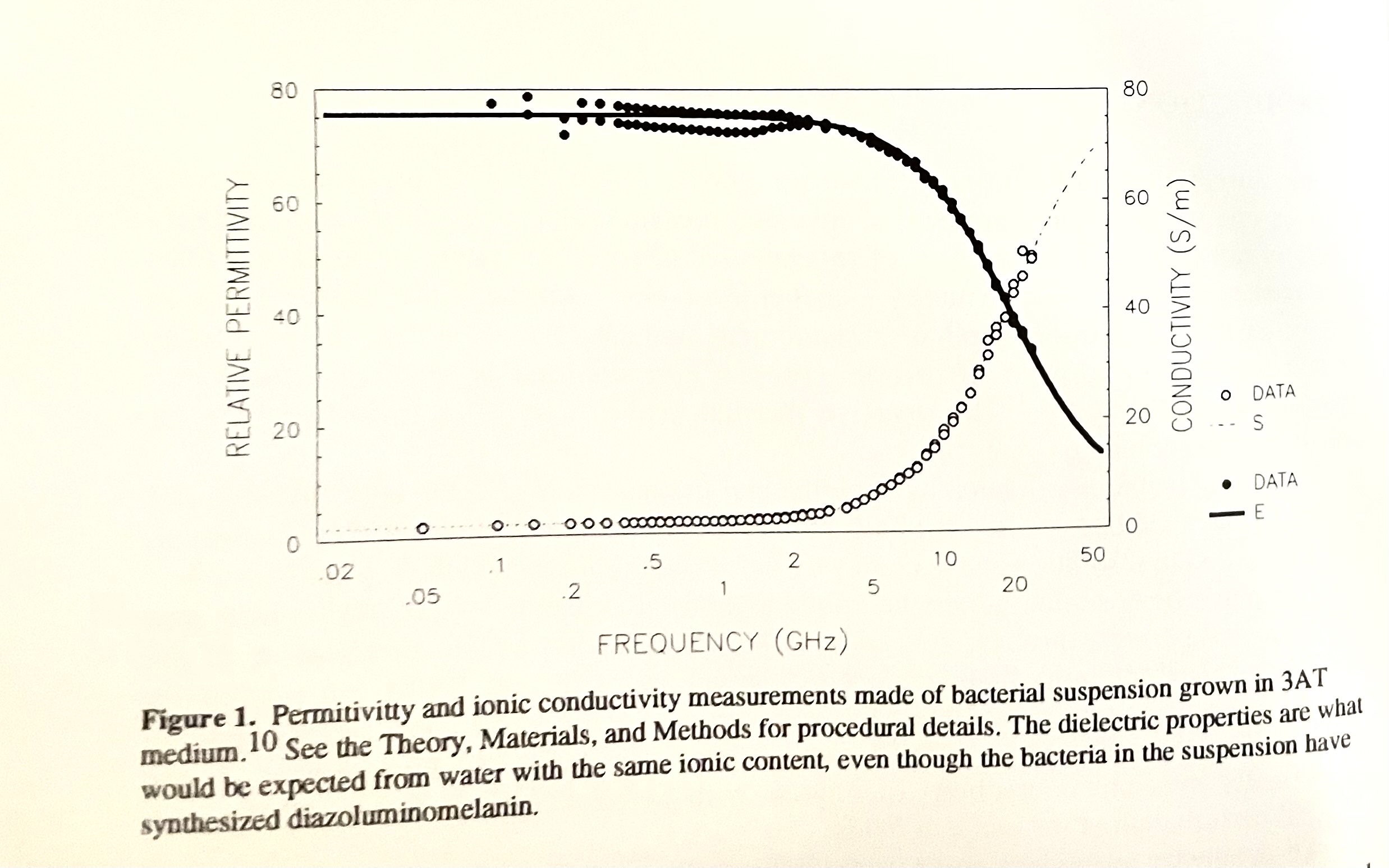
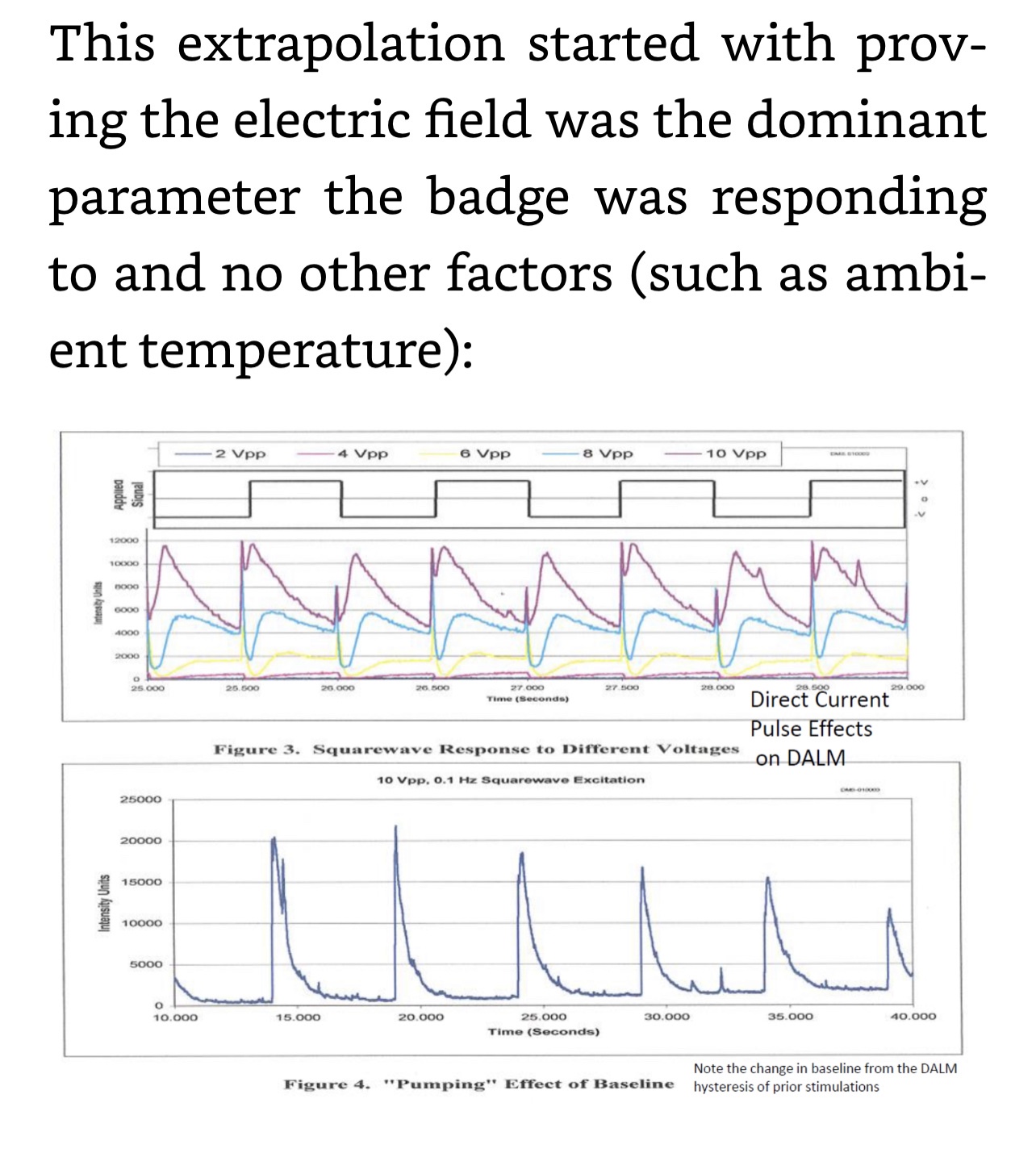
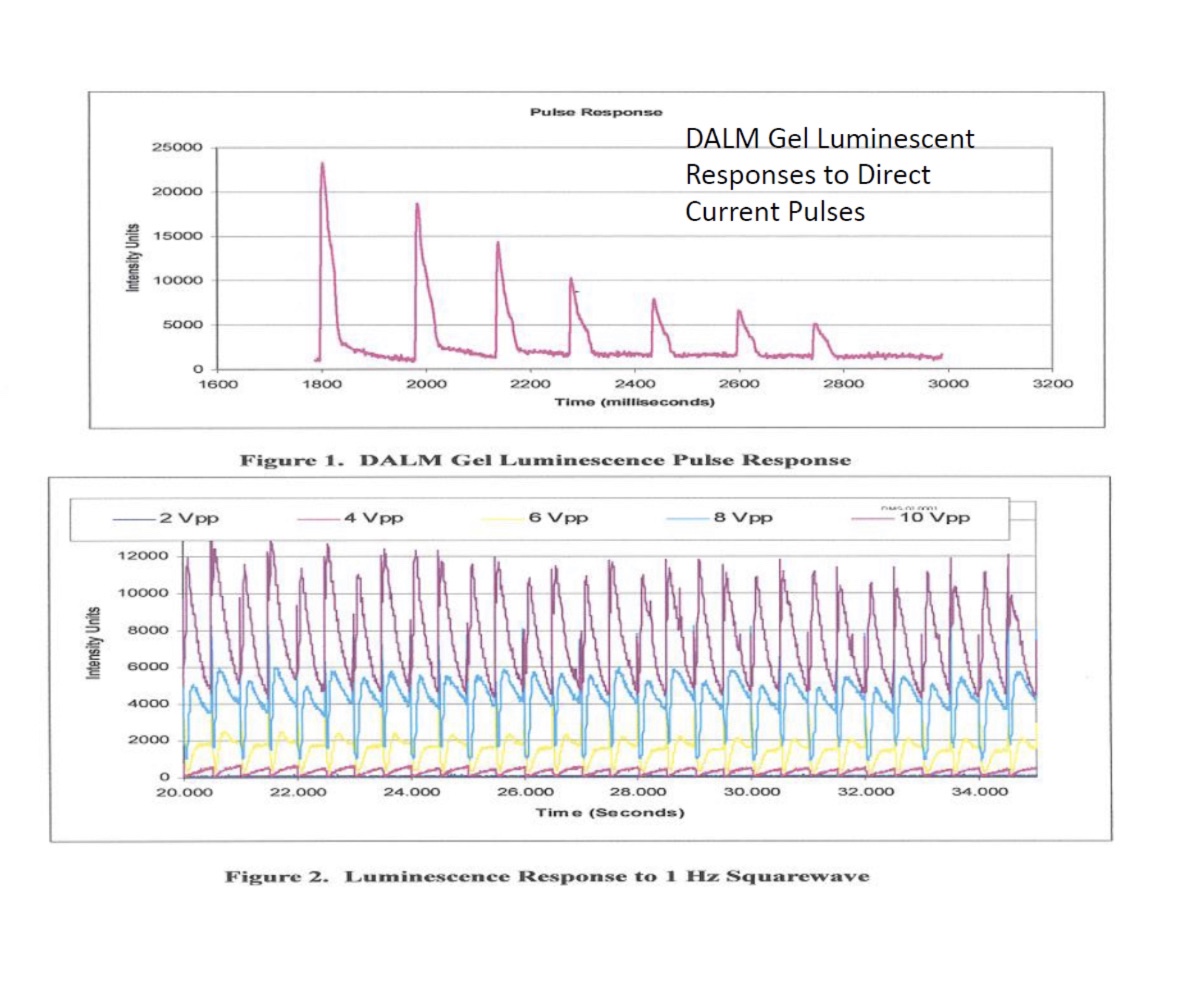
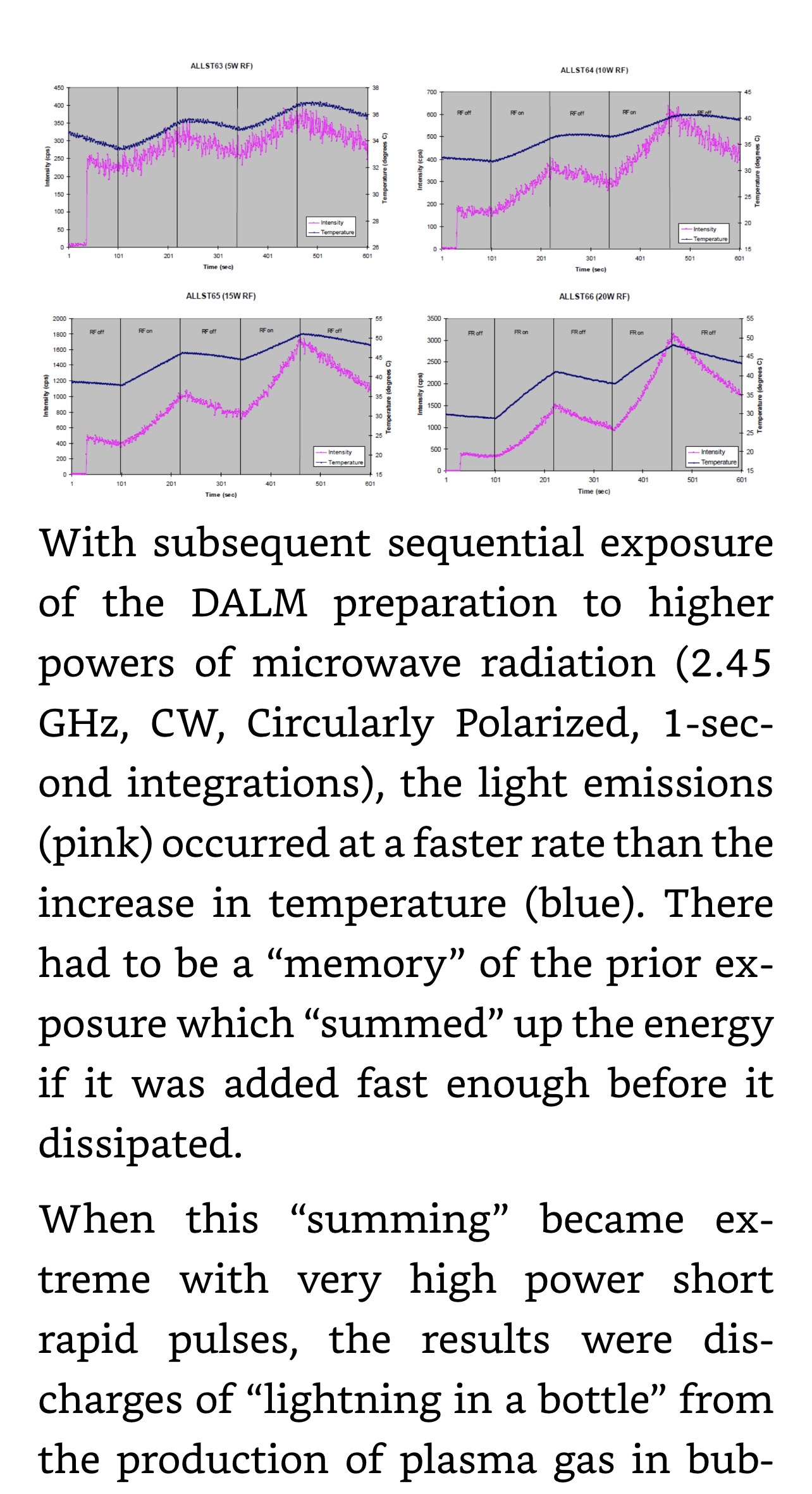
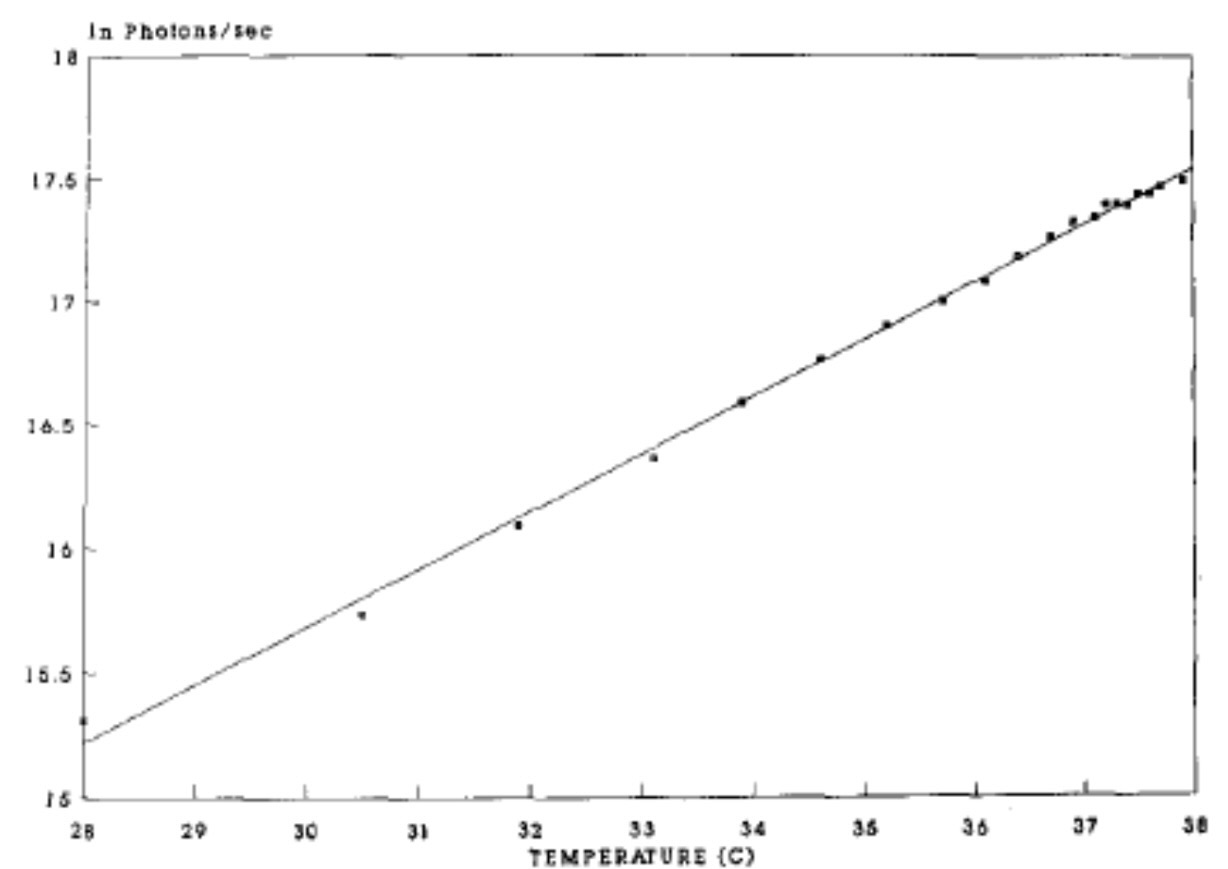
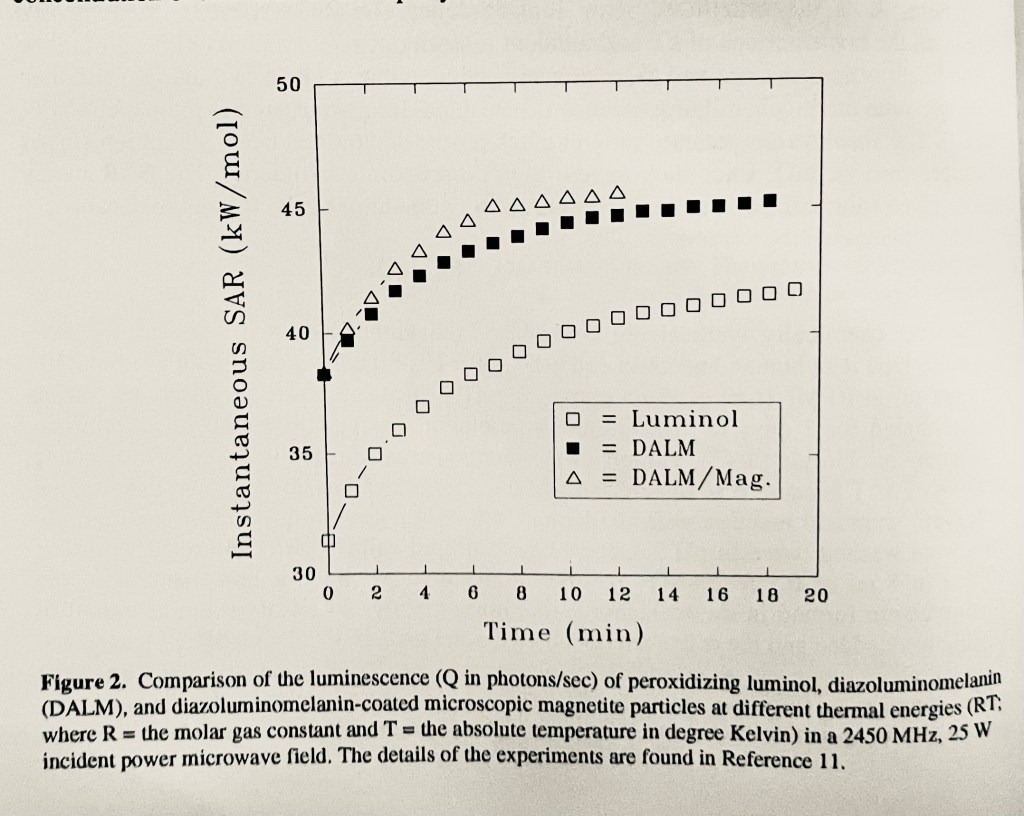
Early on we had observed a very good correlation between luminescence of DALM and microwave heating:
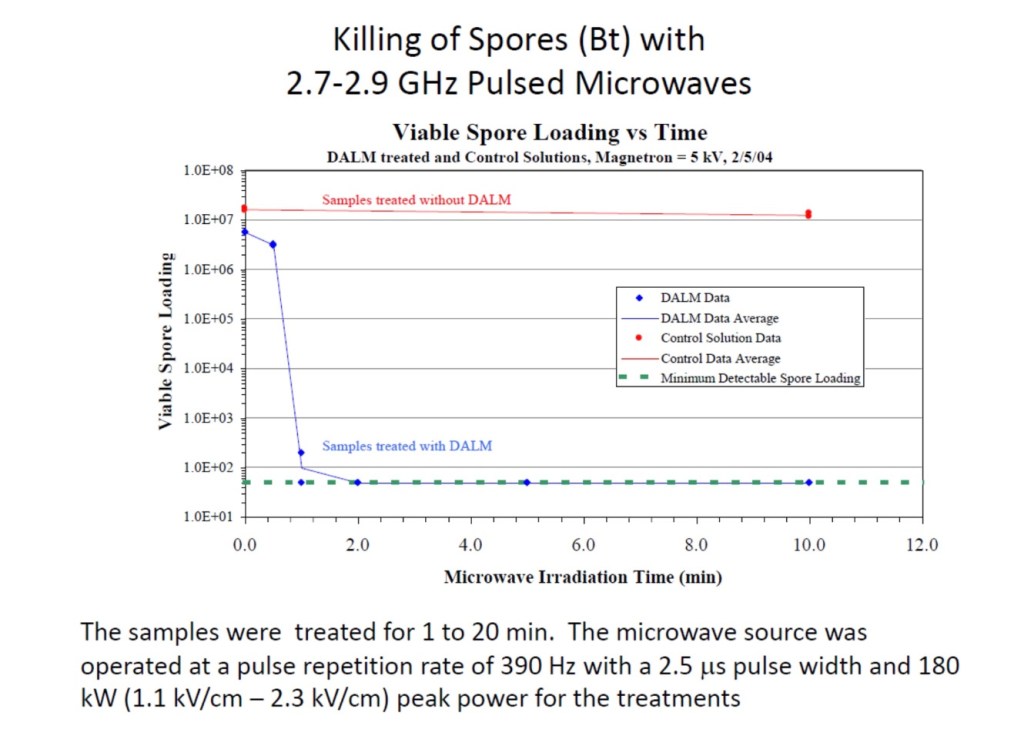
Could these effects still be the result of rapid rise deposition of pulsed microwave energy as thermal energy in an electrolyte solution? First, evidence that was not true was by the above rapid killing of bacterial spores in the presence of DALM by pulsed microwave radiation and the complete absence of effect from the same radiation exposure without DALM.
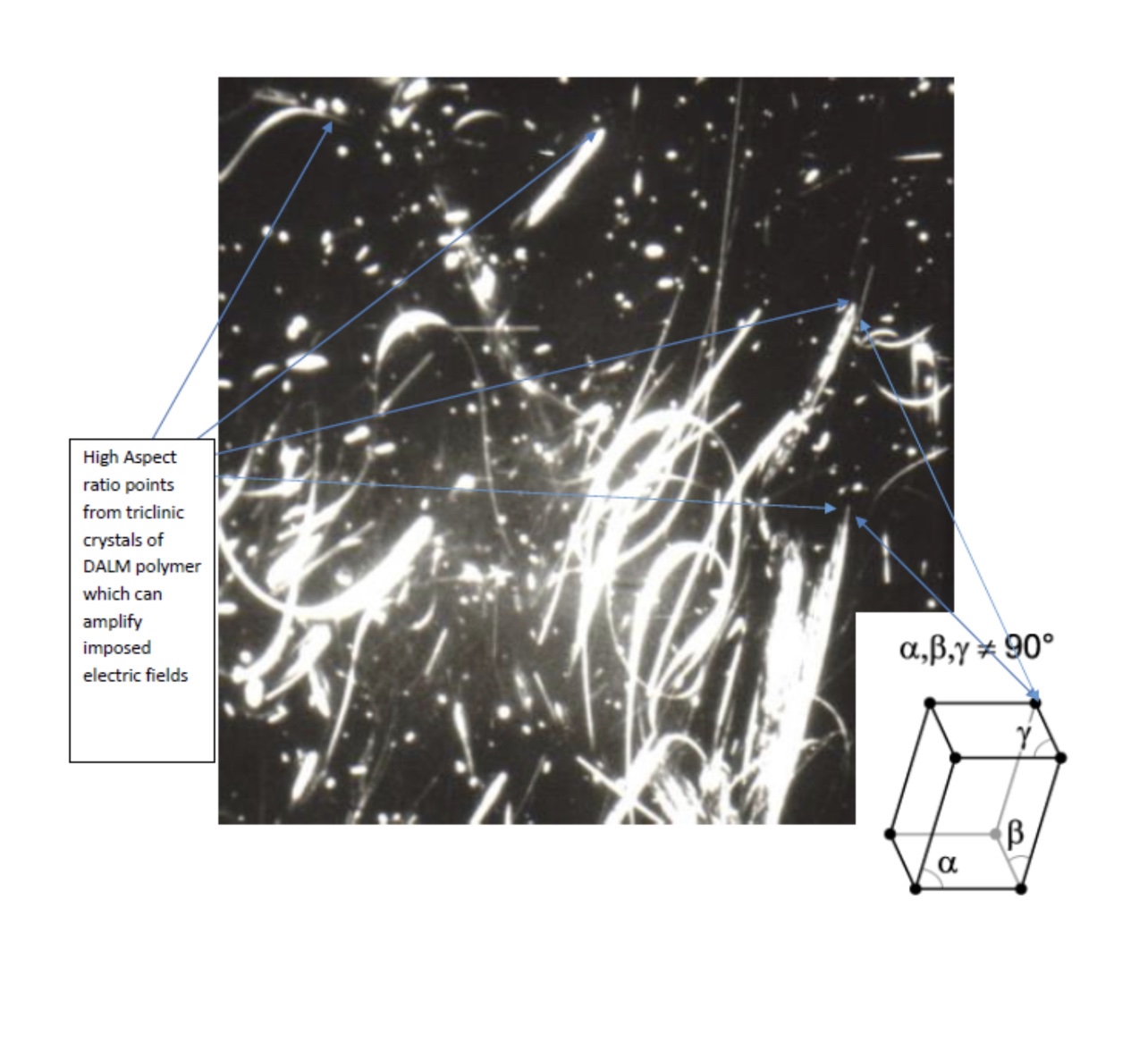
Even the possibility of the DALM fibers focusing the electric fields, and therefore, energy deposition, did not hold up to further examination; an even more effective form of the DALM polymer was in the form of spherical nanoparticles:
In our Counterproliferation mission, this result seemed a great advantage, in delivering nanoparticles that could kill bioagents on surfaces and perhaps even in the air, specifically, and controlled by the application of pulsed microwave radiation at levels normally not harmful that, in turn, could be turned on and off at will, reducing collateral damage.
Unfortunately, a countermeasure to biological warfare could be perceived as a bio or chemical weapon, because what can be used against difficult to kill microbial targets could be used most effectively against human “soft” targets. For instance, a halogen bomb (chlorine or fluorine) could be perceived as a chemical weapon to be used against people or a weapon to destroy highly pathogenic biological weapons,

Such technology, as discussed here, could easily be employed as biotechnological weapons, even if intended to counter bioweapons, could have untoward effects or nefarious use. I presented a paper at the Twelfth Annual Directed Energy Symposium, 2-6 November 2009, San Antonio, Texas, titled “Biotechnological Nanowarfare: Directed Electromagnetic Energy Control” which warned: 1) Chinese and Russian researchers follow our (Brooks Team) research on genetic engineering of microbes and animal/ human cells and their interactions with directed energy. 2) The Chinese are hotly pursuing aptamer development, biotechnological manipulation and nanoparticle delivery systems, especially for the brain. 3) Even if we never make Nanobes, we will have to face them.
There are things apparently potentially worse than pandemic COVID, conventional bio and chemical warfare, GMO pathogens, or pathogenic microbes that escape high containment laboratories. The building of a synthetic anti-microbial nanoparticle that could adapt to and destroy these threats, led to a potentially greater threat in itself. Its further ability to biosynthetically replicate and be adapted to new targets under austere conditions (autonomously?) made it even more of a potential dual use threat. COVID has demonstrated why the Chinese, and perhaps the Russians, want to replace “natural” biological warfare agents with biotechnological ones—backfire.
Chinese military ambitions, were first described in Military Review, July-August 2005 by Guo Ji-wei and Xue-sen Yang. Paraphrasing what these goals are: (1) Crypticity: Biotechnological Warfare is convenient, easy to use, has a small logistics tail (very prone to Terrorist or Special Forces use); (2) Controllability and recoverability: Can be used to measured effect from kill to non-lethal with the option to offer “mercy” in exchange for surrender; and (3) Biotechnological vs. Biological Weapons: Biotechnological Warfare should not be considered Biological Warfare and side-steps any international law or treaty restrictions. Specific quotes from this article make the intent perfectly clear and, furthermore, its use to neutralize certain unruly elements within the borders of China: (1) “If we acquire a target’s genome and proteome information, including those of ethnic groups or individuals, we could design a vulnerating agent that attacks only key enemies without doing any harm to ordinary people. We could also confine the attack to a more precise level. Injuries might be limited to a specific gene sequence or a specific protein structure. Through gene manipulation, we can attack or injure one or more key human physiological functions (the ability to learn, memorize, keep one’s balance, or perform fine motor activities and even act aggressively) without a threat to life.” (2) “If we determine the relationship between the specific frequency, wavelength, or power of the ray or wave and the specific gene or locus, we can cause injury by remote, radiation-induced, genetic function changes.” (DALM Nanobes provide a range of available electromagnetic radiation to achieve this goal).
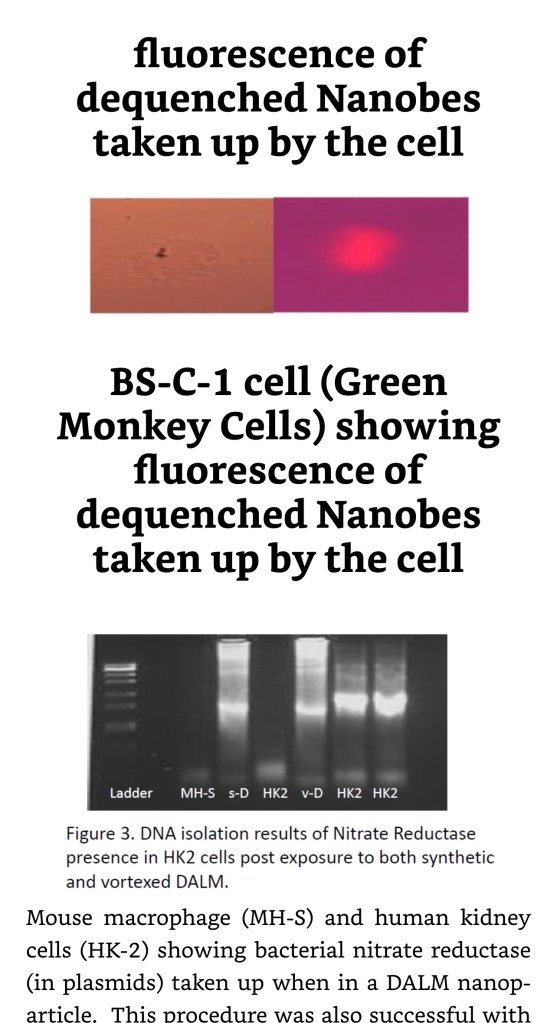
The uptake by a wide variety of cells, prokaryotic and eukaryotic, from bacteria to human cells, with demonstrated capability of genetic modification, if lethal RFR or microwave radiation is not applied, has raised the possibility of nefarious use. Further, the very genetic modification so these cells could produce biosynthetic DALM and transfer the genetic material to more naive cells, could amplify and spread susceptibility to more cells, tissues and organs. Some benefits of self-replicating synthetic nucleic nucleic acids are now being revealed in response to COVID: Bloom, K., van den Berg, F. & Arbuthnot, P. Self-amplifying RNA vaccines for infectious diseases. Gene Ther 28, 117–129 (2021). https://doi.org/10.1038/s41434-020-00204-y.; and Int Immunopharmacol. 2021 Dec; 101: 108231. Published online 2021 Oct 7. doi: 10.1016/j.intimp.2021.108231. See “First self-copying mRNA vaccine proves itself in pandemic trial: Twist on current vaccines reduces dose, eases distribution by Jon Cohen, Science: page 446, 29 APRIL 2022, VOL 376 ISSUE 6592.
However, self-replicating translatable viral RNA has its dark side (the following data were collected by the Brooks AFRL Counterproliferation Team in 2000):
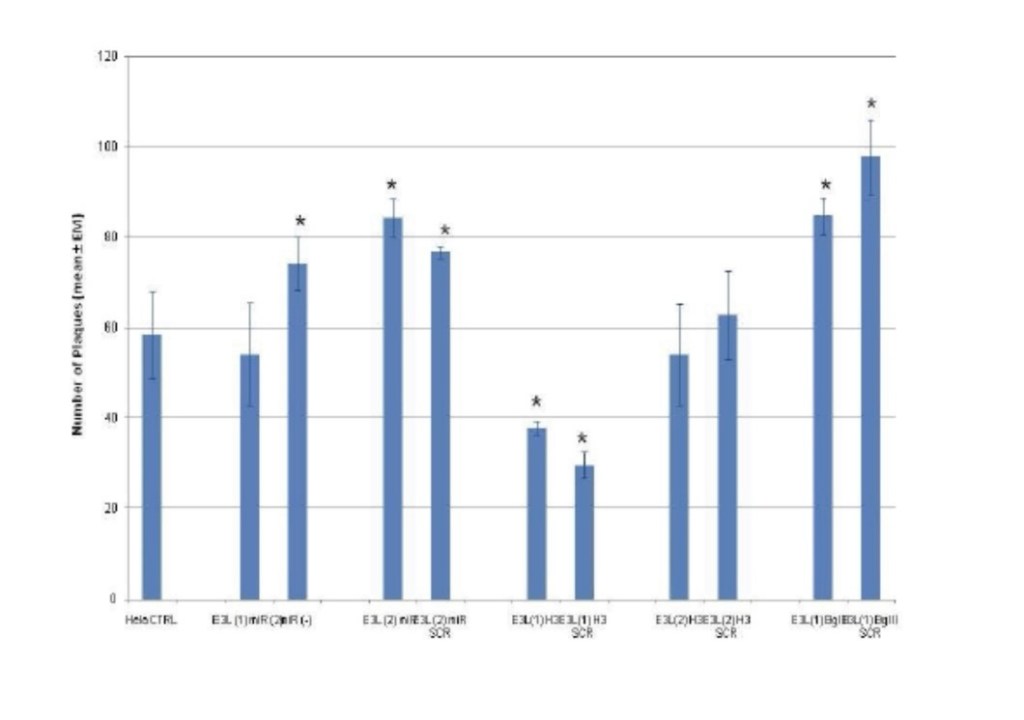
“The small and simple VEEV has one more trick which it shares with the plant Tobacco Mosaic Virus; it can resurrect itself from broken pieces. The nsP4 sequence in VEEV is very similar to the replicases of three plant viruses, including Tobacco Mosaic Virus. The Brooks Lab performed a critical experiment using the RetroXpress( TM) system of Clontech derived from a retrovirus which could transfer genes but could not infect and replicate, my group at Brooks constructed a new virus that contained the nsP4 sequence inserted into this platform and expected that the new virus could infect cells but not replicate. It not only infected (transfected) marker genes into the target mammalian cells but also formed plaques of transformed cells (those which resembled cancer cells and formed uninhibited growth mounds of cells). These grew and multiplied in the cell culture. A new complete infectious virus had formed. How? Tobacco Mosaic Virus has been shown to repair and reactivate after exposure to UV with the help of an unknown plant nucleic acid repair system. Since we inserted only the nsP4 protein into the host cells co-infected with the defective retrovirus, we proposed that the new virus used cellular RNA dependent RNA polymerase in conjunction with the expressed nsP4 to form a repair complex which constructed a chimera virus from the retroviral pieces and other unknown viral nucleic acid components inherently present. Perhaps, the infections by killed virus from killed vaccines previously reported were not just because of contamination with whole live virus but with components which survived the formalin damage and were reassembled into whole restored infectious virus, albeit at a less effective infectious dose of original broken pieces. Intact VEEV will produce a transmissible infection with as little as 12 PFU (plaque forming units equivalent to 10 virions for a multiplicity of infection of 1 but more likely 10X10 = 100 virions). I have speculated that these broken viruses, if reconstituted from broken virions or free RNA would require 10e6 units to make one intact virion.”—The Black Dragon Trilogy by JOHNATHAN KIEL
https://a.co/gLQ6en9
VEEV= Venezuelan Equine Encephalitis Virus, a Select Agent zoonosis.
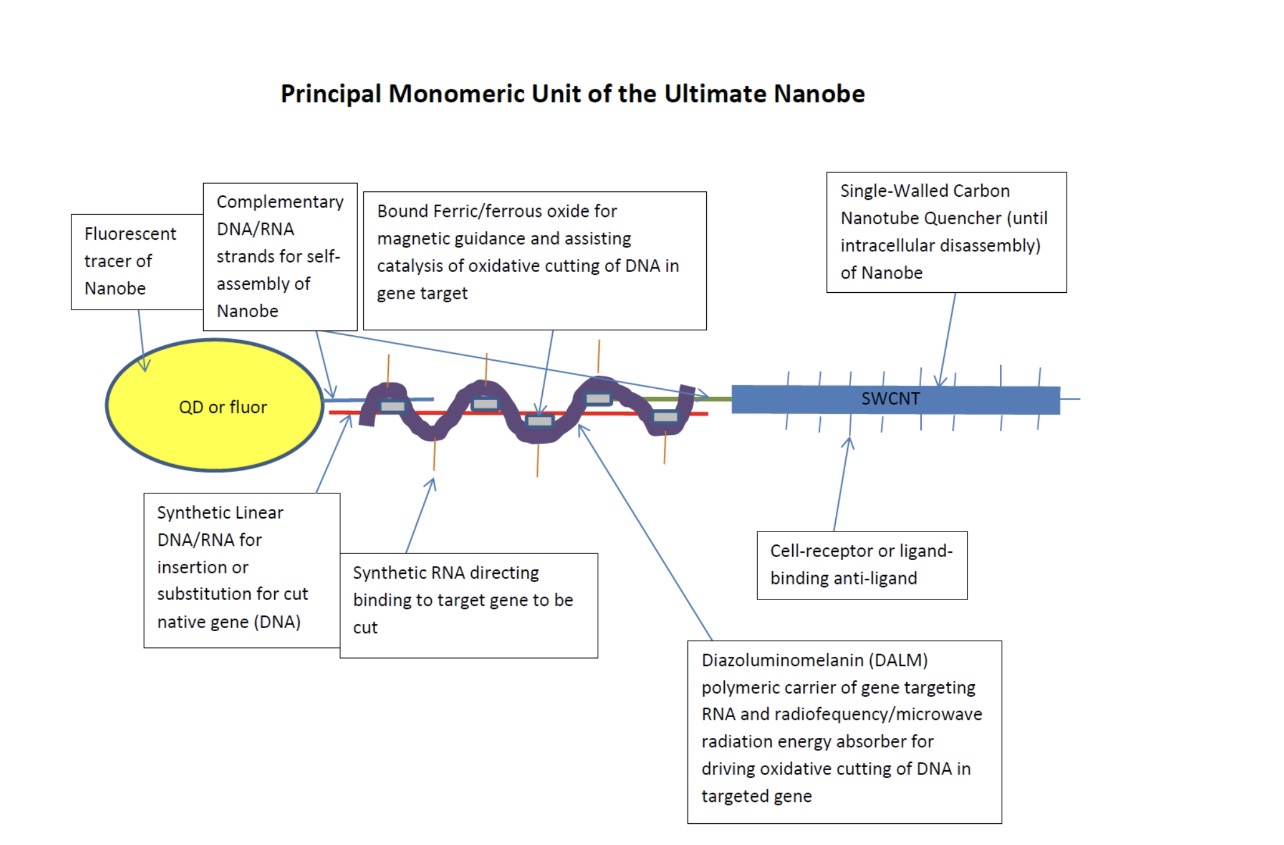
The diagnostic fluorescent tracer format was originally designed to be built on the high aspect nano conductor assumption that also acted as fluorescent quencher, especially of high quantum efficiency quantum dots. It was thought that carbon nanotubes would be required for this function but DALM proved it could do it alone without the apparent high aspect ratio mechanism in nanoparticles.
Thermochemiluminescence (microwave) in other human cells, HL60 cell line:
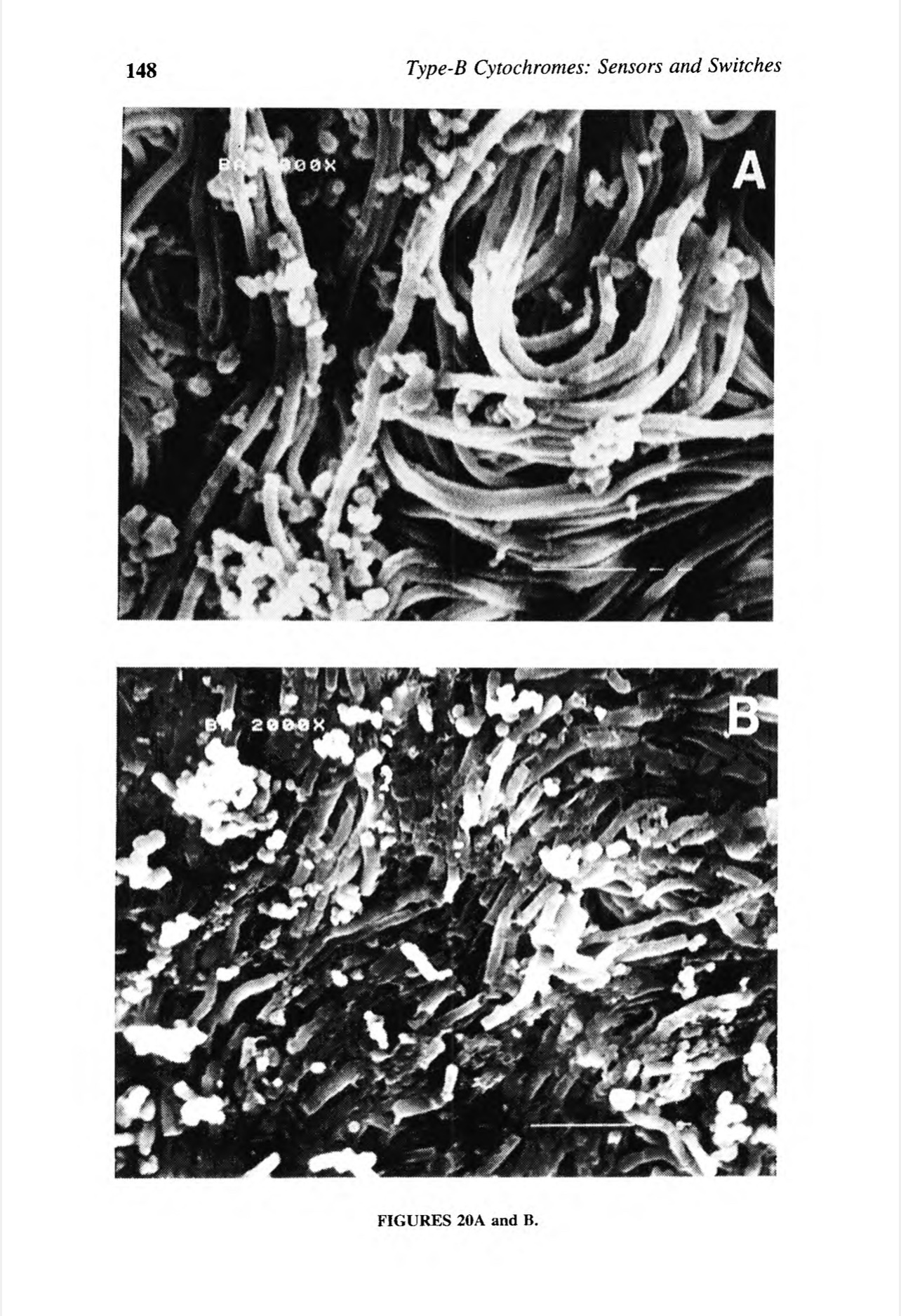
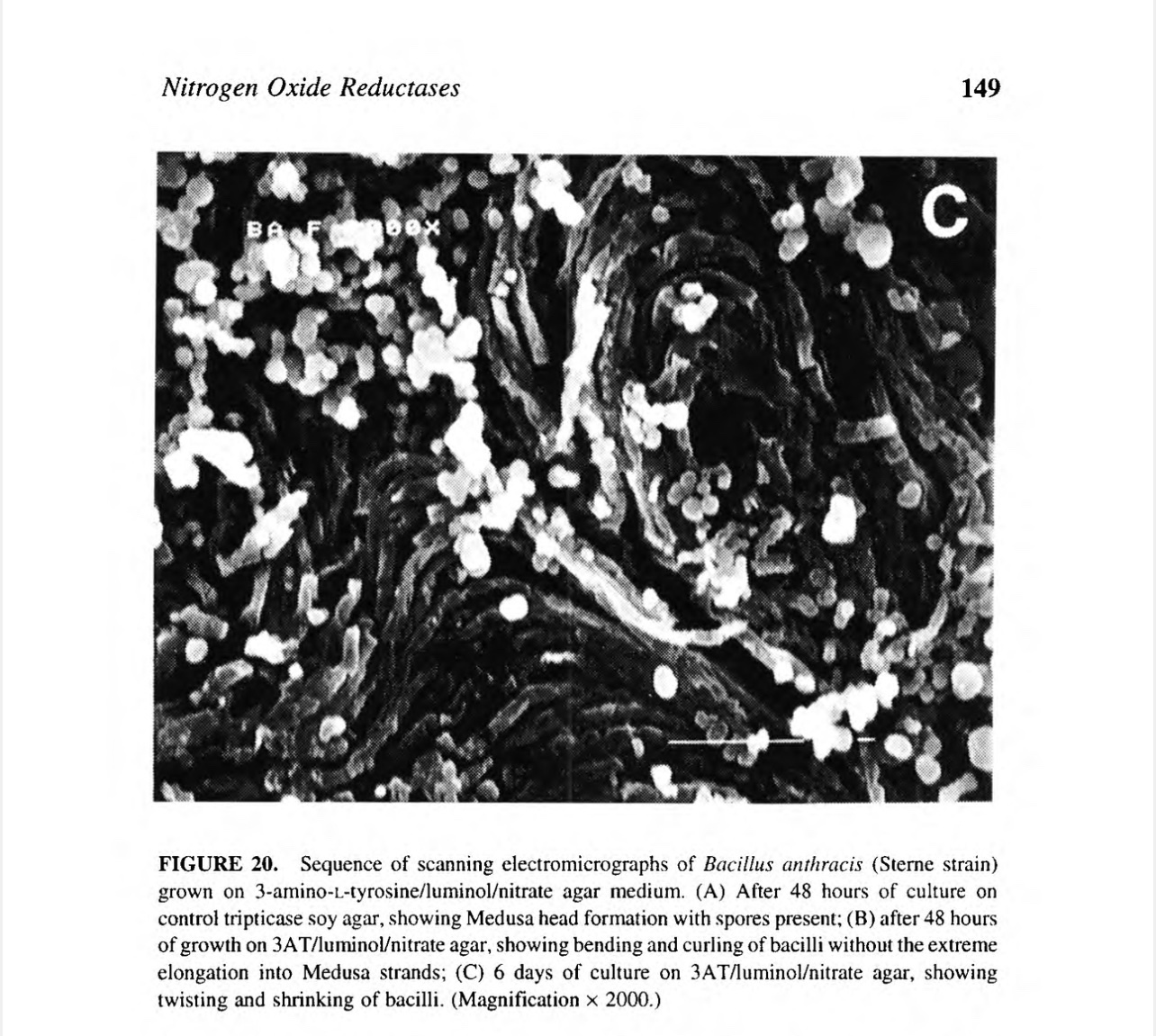
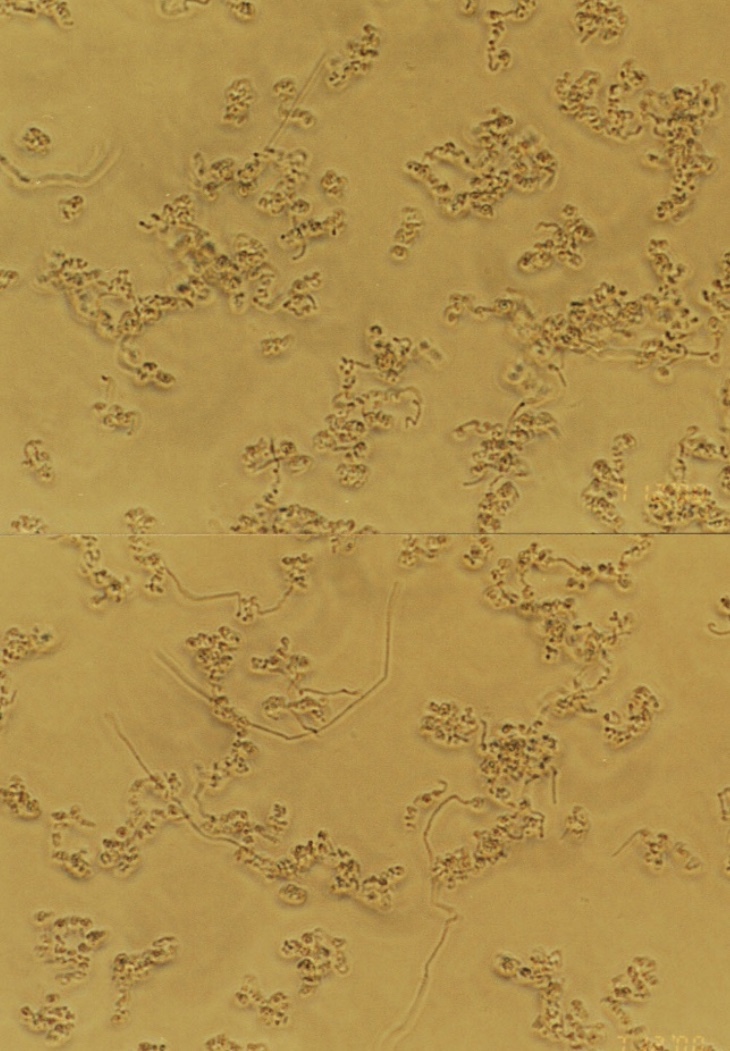
The coiling morphology induced in anthrax bacteria in medium that induces DALM biosynthesis:

The second problem to solve was delivery. Nanoparticles can be and have been easily delivered by small nanosprayers. One gram of such particles can be distributed into a 10m X 10m X 1km volume, maintaining a concentration over 2 million particles per cubic centimeter. This is a formidable weapon easily transportable.

The third problem solved by the DALM nanoparticles was directing the effects to specific tissues and organs. Chinese investigators have demonstrated in animals nanoparticles can enter the brain through the nose and localize in specific parts of the brain (Wang J, Y Liu, F Jiao, F Lao, W Li, Y Gu, Y Li, C Ge, G Zhou, B Li , Y Zhao, Z Chai and C Chen. 2008. Time-dependent translocation and potential impairment of central nervous system by intranasally instilled TiO2 nanoparticles. Toxicology doi: 10.1016/ j.tox. 2008.09.014). They may also enter the auditory organs through the nose and Eustachian tubes or via the auditory nerves in the brain.
The Havana Syndrome (first observed in 2016 amongst US diplomats in Havana, Cuba) is manifested by a range of symptoms including dizziness, headache, fatigue, nausea, anxiety, cognitive difficulties and memory loss of varying severity. In some cases, diplomats and intelligence officers have left active service due to complications from the condition. Was and is it caused by pulsed microwaves? The CIA reported there was no evidence linking Havana syndrome to a foreign country (January 20, 2022 · 9:43 AM ET NPR. Greg Myre National Security Correspondent). Really? That doesn’t say it wasn’t done by a foreign power. It means that they don’t know or won’t tell.
“The question remains: whether the auditory effect can be “weaponized,” i.e., used to harass or harm an individual. For reasons of effect size and practicality this appears unlikely, but the lack of publicly available information about existing high power RF technology and uncertainties about thresholds for adverse effects does not allow full resolution of the matter” (Foster KR, Garrett DC and Ziskin MC (2021) Can the Microwave Auditory Effect Be “Weaponized”? Front. Public Health 9:788613. doi: 10.3389/fpubh.2021.788613). Hamlet: “There are more things in heaven and earth, Horatio, than are dreamt of in your philosophy’
The use of DALM nanoparticles clandestinely first delivered to targeted individuals then generalized exposure to a RF source would lower the threshold of bioeffects on selected individuals and spare the rest (unnoticed) who were RFR exposed. This enhancement would greatly reduce the required size of the transmitter and the limitations on the frequencies because of depth of penetration and power requirements. Once triggered these nanoparticles may trigger residual effects without additional RFR exposure, meeting Dr Foster’s et al requirements for “weaponization”. The Nanobe (DALM metallic nanoparticles)/pulsed microwave potential weapon is like a combination of Mission Impossible films 2 and 3, Chimera and the RFR exploding pellet in the brain, art follows science, fiction fact. Where is Bellerophon? In the Jurassic Park film Ian Malcolm says emphatically, “Your scientists were so preoccupied with whether or not they could, they didn’t stop to think if they should.” Or perhaps who should be allowed to do it and for what reasons? Who should decide? It’s all about intent.
This post serves as a preview of my new book, Bionanotechnology, coming out soon from Springer Nature (to be completed 4 Sept 2024) that explains this technology in detail. The only commercial source of bionano-formulations of DALM at this time is the J&R Project (https://contest.techbriefs.com/2022/entries/medical/11693). These formulations are necessary to optimize the light and sound effects. Don’t lose heart, “Something wonderful” is about to happen.
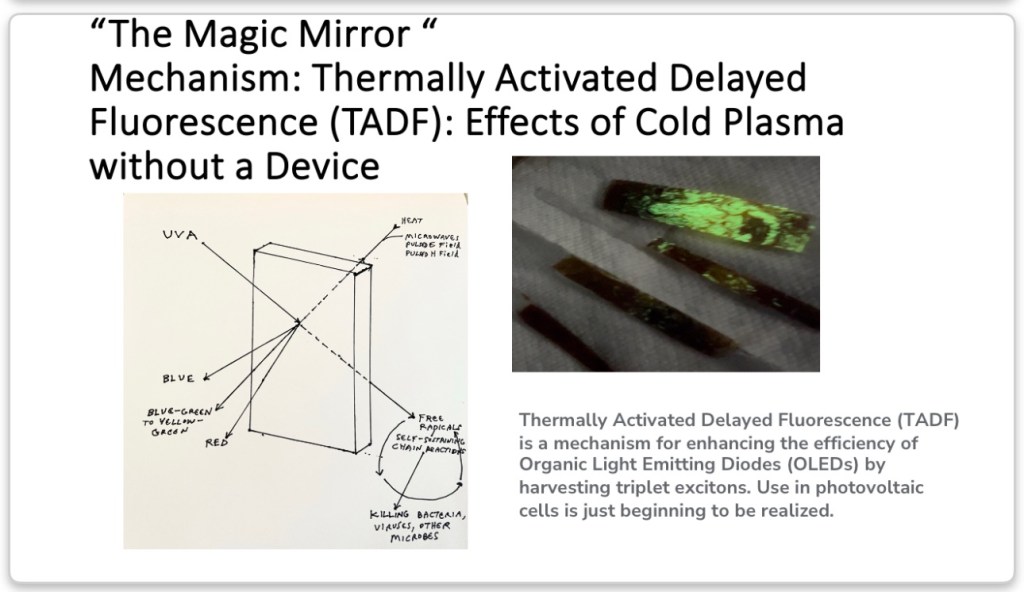
Maximized DALM Thermally Activated Delayed Fluorescence



The End
Recently, SARS-CoV-2, COVID, has shown that it has more surprises for us. The following diagram is based on the comparison of all the genomes of SARS-CoV-2 isolates grouped into related variants. The South African recent isolate variant (red lines) did not evolve from other current variants. The 91 genomes from Omicron viruses (@GISAID) were from specimens collected between Nov 11 and Nov 23 in Botswana, South Africa and Hong Kong. On 26 November, the World Health Organization (WHO) designated SARS-CoV-2 variant B.1.1.529, as a variant of concern and named it Omicron, on advice of scientists in the WHO’s Technical Advisory Group on SARS-CoV-2 Virus Evolution. Omicron was added to WHO list of current variants of concern: Delta, Alpha, Beta and Gamma. The Omicron variant has a high number of mutations especially in the spike protein. The extremely long red branch (>1 year) below indicates an extended period of circulation in a highly localized geographic area with poor genomic surveillance (not in South Africa proper but some contiguous or connected area by travel) or continual evolution in a chronically infected individual before spilling back into the population. It is not likely an animal source, as some have suggested, but has a peculiarity of one coronavirus, feline infectious peritonitis virus, in particular, that has been observed for many years and in another, originally zoonotic virus, that has been maintained in a slow but enduring pandemic, HIV.
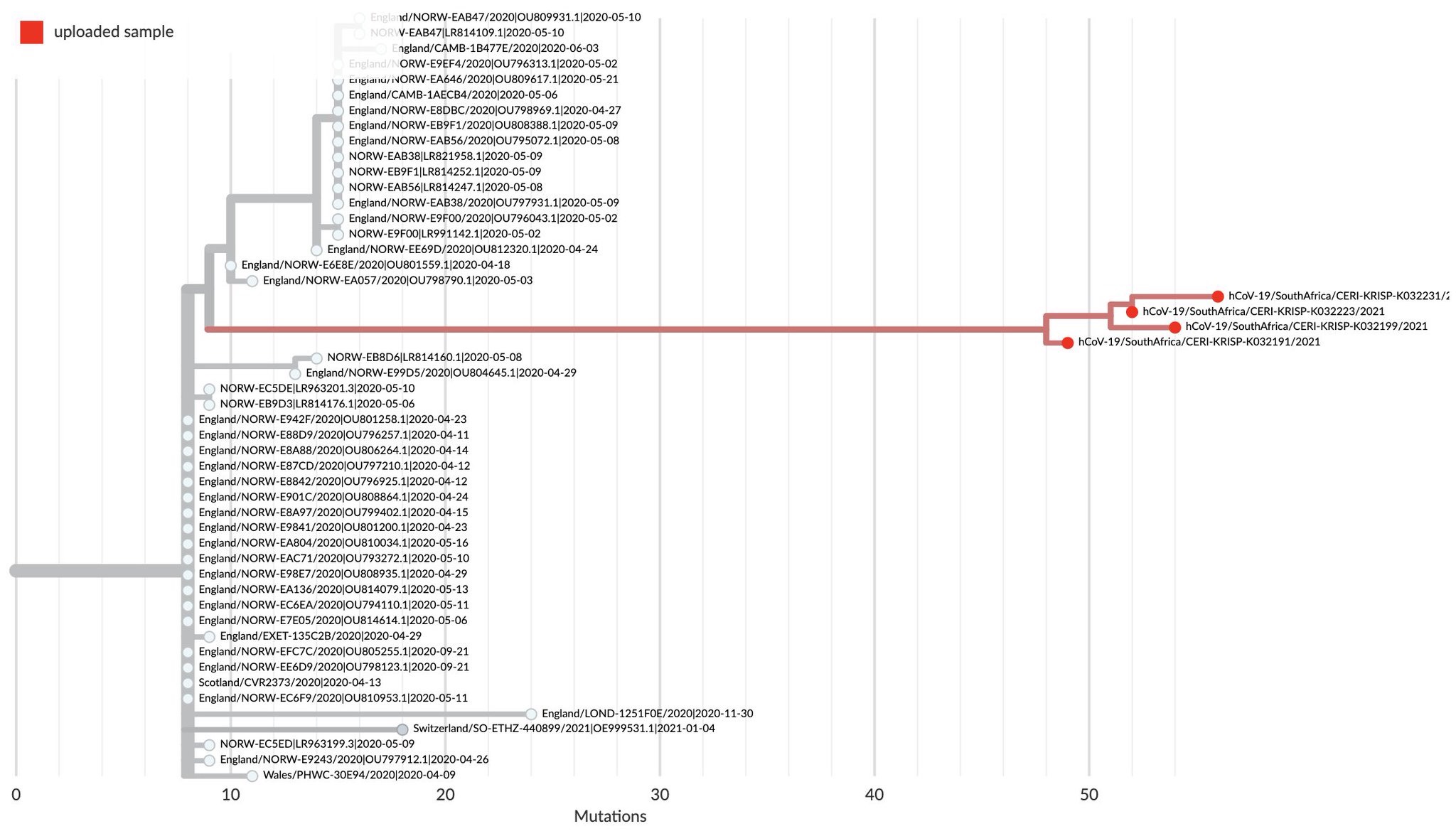
The sources of this diagram are https://twitter.com/trvrb/status/1464353224417325066?s=21 and https://www.pango.network/.
For these changes to occur in such isolation, mutations forced by natural selection in a small number of hosts or in a single host, there must be one or more mechanisms of immune evasion and survival of the host(s) to allow for the time for these mutations to occur and to select for survival of the virus. How could one get Omicron variant ? Two CoVs could infect the same cell at once and share genetic material to make a new virus (homologous recombination). HIV generates mutations frequently, even within the same individual, because of the sequence mistakes made by reverse transcriptase, which converts the RNA to DNA, which is, in turn, inserted into the host genome from whence it is expressed as new virus. Even though coronaviruses have a proof reading RNA dependent RNA polymerase, they still make mistakes in replication, and mutations are also produced in the viral RNA templates by the active oxygen and nitrogen compounds produced by inflammatory cells which produce chemical changes in the RNA nucleotides which alter replicated sequences. The viral selection process is driven by the host immune system against the frequently changing protein structure, eliminating the variants for which it is specific and leaving behind the evading ones to enter new host cells and replicate. The anti-parasite immunity described in earlier posts may also be, at least in part, responsible in allowing the SARS-CoV-2 time to mutate and escape the immunity in a single host. This is seen in such parasitic diseases as African Sleeping Sickness (trypanosomiasis) and malaria, and may even produce a stalemate with the host called premunition, infectious immunity ( https://www.frontiersin.org/articles/10.3389/fimmu.2019.02738/full). It appears SARS-CoV-2 has chosen to enhance anti-parasite immunity like that used by the hosts to control parasitic worm, pathogenic protozoan and fungal infestations and infections. This response often controls the number of parasites to a tolerable, but not immediately lethal, level and prevents further infestation (process premunition), but does not totally eliminate the parasite. But is there any precedent for this in other coronaviruses in animals?
Cats get an enteric coronavirus which has little or no signs, but, in certain young cats, it becomes disseminated, causing peritonitis with lethality, usually 100%. Cell-mediated immunity provides an effective immune response that resolves the infection in the enteric, intestinal form. If it does not, a strong humoral response kicks in and selects for a more pathogenic form of the virus which infects and replicates in macrophages https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7112361/pdf/main.pdf. Also, autoantibodies form. There seems to be genetic predisposition toward this resulting in peritonitis https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2819880/. Peritonitis pathology involves severe systemic inflammatory damage of serosal membranes and widespread pyogranulomatous lesions in the lungs, liver, lymph tissue, and brain. The clinical finding of hypergamma-globulinemia-associated feline infectious peritonitis is indicative of over production of antibody against an antigen which cannot be cleared, allowing time for viral mutations that allow the virus to escape elimination. Therefore, like COVID-19, the feline coronavirus virus disease has this dichotomy, based on viral dissemination and autoantibodies. The right antigen for the right vaccine must be selected to prevent such adverse effects.
SARS-CoV-2, continues to evolve by mutation and selection toward being more efficient at infection and transmission within close, tight social groups but falling off quickly when vaccination and moderate barriers, like masks and good ventilation, and social distancing are implemented.
Vaccination does NOT guarantee protection from infection by Delta, Omicron, or any new variant or transient release of virus from asymptomatic vaccinated individuals. Vaccination is NOT for elimination of all possible virus but to reduce infection level below the point of symptoms of disease in immunized people (varies from person to person somewhat, but is more likely to be overcome with higher circulating viral loads). It is the circulating of more infectious particles over and over so there can be accumulation and increased probability of developing more mutants, therefore, variants, that is problematic. Omicron is just SARS-CoV-2 testing the perimeter for weaknesses.
The first Omicron case has arrived in the US in California in a person returning from South Africa Nov 22. Fully vaccinated, this person has displayed mild symptoms, is in quarantine, and all contacts tested have been negative so far (CDC).
It now appears that long term carriers, with few or no symptoms of SARS-CoV-2 infection do exist in humans. Recently, researchers from the Pasteur Institute (France), University of Sao Paulo and Oswaldo Cruz Foundation (Brazil) have reported a 38-year-old man continued to test positive for coronavirus COVID-19 for at least 232 days. He has had HIV since 2018 but with no detectable virus because of antiretroviral therapy. They also showed others who had been infected for up to 70 days (https://url2151.isid.org/ss/c/TLh_csrC34X_iXpbYoMam9YStmt7vu-BzT2xitPooDV_2a0YcE0beocoTmJzw1B0i0POJ_295MZ7M7WB4SUhI8W3O6cwWl0KateCaan9KY8/3j9/zgJqdfMITpyHJ-pA-wvf7w/h4/jiqEWCKMtqTr1a6jNj2OgFklAK0eY27ry_9eZGm70WU).
This analysis is based on past experience and studies applicable to SARS-CoV-2, and the Omicron variant in particular. I still maintain that SARS-CoV-2 is an animal virus, a generalist, and opportunist with an imposed human bias. It has kept its options to infect and be maintained in animal species other than humans. Humans have just provided a profound opportunity for viral amplification and transmission with travel, global contact, disregard for sanitary precautions, socioeconomic disparity (poor vaccine distribution and preferential access to life saving treatments), and political interference (positive and negative influence). Omicron can be viewed as the natural evolutionary progression of the virus under these circumstances. Recent data have shown the first indications that Omicron is following an animal coronavirus pattern that I have described in several earlier posts. The confusion in the press and the debate amongst the scientific community over Omicron being more transmissible (clearly) and less pathogenic (awaiting more data) is an unclear relationship, if any connection at all, between pathogenicity (morbidity and mortality) and transmissibility. Transmissibility seems to follow a logical course of higher transmissibility leading to greater incidence and prevalence of a variant like Omicron, but it has its limitations. Transmissibility is not linear but asymptotic in its evolution. Too much transmissibility and vulnerable hosts become harder too find; too little and the virus infectivity dies out with distance between and immunity of hosts. An inhibition of immunity by the virus leads to greater viral production and lower infectious dose, but too much and the virus spreads throughout a host’s tissues that leads to incapacitation (limited mobility for viral spread) or lethality (eliminating a viral host for replication and spread); too much or too quick induction of immunity and not enough virus is available for transmission. These are the tensions pulling on virus mutations, governing its evolution.
Omicron has, in a preliminary study, shown a preference for infecting human upper respiratory tissue over lung tissue in culture. The omicron variant multiplies about 70 times faster inside human respiratory tract tissue than the delta variant does, according to a University of Hong Kong report (https://www.med.hku.hk/en/news/press/20211215-omicron-sars-cov-2-infection?utm_medium=social&utm_source=twitter&utm_campaign=press_release). This is supported by the fact that, in the U.S., cases caused by the Omicron variant jumped seven times in a week, from 0.4% to 2.9% total cases, according to Centers for Disease Control and Prevention estimates. The infection incidence is approaching 13% of cases in the region including New York and New Jersey. This is close to the prevalence of other coronaviruses in animal populations at any given time (10-15%). The preponderance in the upper respiratory tract (including bronchi) assures large amounts of virus will be expelled with coughs and sneezes and will most likely take hold in exposed susceptible people. Localized immunosuppression in these tissues before recovery is more than adequate to rapidly reproduce and provide time to spread the virus. No increase in pathogenicity is necessary.
However, a shift from preference for receptors deep in the lungs to those of the upper respiratory tract assuring more likely human to human transmission has been seen before in influenza. Avian influenza prefers deeper receptors in the human respiratory system and is more pathogenic. When it reassorts with other strains like those of pigs and humans, it becomes more transmissible in these species, mostly less pathogenic, but not always and without assurance of such a result. So no assurance of Omicron’s decrease in pathogenicity.
The increase in lethality of an infectious entity is often indifferent to transmissibility, especially if it is quick and a living host is not required to spread the agent. Sometimes the dead are a greater source of transmissible agent than the living and the agent is thus selected for lethality as it mutates or against attenuation that would allow recovery and elimination of the infectious form. This situation describes anthrax that is transmitted through spores that form upon death and dismemberment of the host. Even Ebola, until recently, was most likely to be transmitted from person to person by preparation of the dead for burial. Today, not just the dead and dying transmit it but also the recovered through chronic infection and sexual transmission. Its nature has changed as it has moved from being an East African sporadically occurring zoonoses to an endemic urban virus in West Africa. SAR-CoV-2, like other animal coronaviruses, is not so infectiously persistent in the environment, but rather spreads through constantly maintained susceptible populations and by acute and chronic viral shedders (in animals, mostly by the GI tract, yet to be fully demonstrated in human hosts infected with adapted coronaviruses). Time will tell if SARS-CoV-2, Omicron in particular, follows this well tread coronavirus path.
Did Omicron come out of animals? Sequences shared with coronaviruses in rats (https://media.nature.com/original/magazine-assets/d41586-022-00215-2/d41586-022-00215-2.pdf). Spreading to hamsters then back to humans (https://deliverypdf.ssrn.com/delivery.php?ID=905122026003114127079123119001002108070000006036012087096100017005026012108069005085117079006123024016028096075124024095120029035039092080082014103069087050015051047119025019073007018096068101116122057113095048023013018003005127004003074071116075102028010112004123113020012112075020103113022&EXT=pdf&INDEX=TRUE). We have recently seen that even Omicron is mutating toward more transmissibility (Omicron Subvariant 1.5 Times More Contagious Than Omicron: https://www.medscape.com/viewarticle/967541) but not necessarily more pathogenicity, following the course predicted in an earlier version of this posting. Are we approaching the asymptotic maximum?
Isn’t it time for a totally new approach that is both specific and versatile? An approach that can be applied immediately before an emerging infectious disease goes pandemic? A means to “out evolve” a virus or antibiotic resistant bacteria or other microbe before it escapes its origin ? Yes, Nanobes . “I’ve seen things you people wouldn’t believe….all those moments will be lost in time like tears in the rain”.
How can symptoms of COVID-19 persist after the virus is gone? The answer may lie in the type of immune response triggered by SARS-CoV-2, which resembles one more familiar to those studying the immune response to worm and protozoan parasites. I mentioned this in earlier posts citing observations of clinical characteristics of COVID and how they resembled the response to a parasite rather than a virus. Parasite immunology more closely resembles tumor immunology than that of responses to many viruses and bacteria. This cross reactivity between tumor immunity and the immune response to SARS-CoV-2 has been dramatically illustrated in a recent case of a rare remission of advance Hodgkin lymphoma in conjunction with COVID (https://onlinelibrary.wiley.com/doi/10.1111/bjh.17116). The host must mount a different kind of response to parasites because of their many strategies to evade the immune system, the innate and adaptive components. Therefore, animals and humans have developed a different series of cellular and humoral components unique to parasites, but often with potentially severe collateral damage to normal tissues and organs. There is a delicate balance between controlling a parasite infestation so that it does not consume the host and so completely destroying the parasites that the host “burns down the house to get rid of the rats”, auto destruction of the host in the process of eliminating the parasite and confusion between parasite antigen and self antigens (autoimmunity) https://downloads.hindawi.com/journals/iji/2014/651503.pdf. The remaining “memory” of this response, after the virus is gone, is continuously reactivated by a broad range of stimuli https://jlb.onlinelibrary.wiley.com/doi/epdf/10.1189/jlb.0313113. This primitive process, discussed in my book Type B Cytochromes: Sensors and Switches and cited in previous posts, is built on anticipatory responding to potential pathogens, toxins and physical insults before those insults are actually known or specifically identified. This is good for evolutionary survival but can lead to unnecessary overt nonspecific responses and collateral damage. What is the evidence for such a hypothesis in regards to COVID-19 and how might it lead to treatments, especially for long haulers? As stated in a previous post, the immune response of hospitalized COVID-19 patients falls across a spectrum of immune responses in 3 categories: (1) antiviral (some macrophages and dendritic cells, natural killer cells, cytotoxic T cells, helper and suppressor T cells, antibody making B cells and plasma cells, and gamma interferon; other interferons made by tissue cells: alpha and beta); (2) anti-parasitic granulocyte white blood cells (some special B cells that make IgE, eosinophils, basophils (in tissue mast cells), and all kinds of biochemical mediators: histamine, prostaglandins, leukotrienes, and kinins); and (3) anti-bacterial and fungal (granulocyte: neutrophils, and monocytes and macrophages). COVID-19 can move through all three types. The worst and most likely cause of the long hauler syndrome is type 2 which was meant for worms and other multicellular localized parasites and can be locally severe and if generalized, fatal. The serum concentrations of IL-17A (a protein that recruits monocytes and neutrophils to an inflammatory site produced by Th17 lymphocytes) and IFN-γ, but not TNF-α or IL-6 (the pro-inflammatory culprits), decrease with age of patients (this might argue against Th17 memory cells being the source of long haulers); therefore, gamma interferon’s ability to prevent viral replication but not induce oxidative damage to host cells, as with TNF-α, is more important in children’s responses. However, as stated in a previous post, evidence supports decline in soluble IL17A receptors, which block TNF-alpha and interferon gamma production by competing with the cellular T17 cellular receptors, leads to more severe COVID19 (supporting Th17 cell involvement). Adults show a more robust T cell response to the viral spike protein compared to pediatric patients shown by increased expression of CD25+ on CD4+ T cells and the frequency of IFN-γ+CD4+ T cells. Also, serum neutralizing antibody titers and antibody-dependent cellular phagocytosis are higher in adults than in pediatric COVID-19 patients. The neutralizing antibody titer increases with age while the IL-17A and IFN-γ serum concentrations decrease. Children seem to be resistant to the severe effects, except in some instances when they display multiple organ inflammation, Kawasaki-like syndrome, because they produce a lot of the anti-inflammatory cytokine IL10. The responses of neonates compared to adults change from increased IL-10 as neonates to balanced IL-10/T helper type 1 (Th1)/Th2/Th17 cytokine levels early in life. This allows protection from pathogens but reduces the chances of severe inflammatory reaction. Th17 cells are the most probable mediators in many human autoimmune and chronic inflammatory disorders, including psoriasis, Crohnˈs disease, rheumatoid arthritis, Multiple Sclerosis, and uveitis https://www.frontiersin.org/articles/10.3389/fimmu.2018.01112/full. The development of pathogenic Th17 cells relies on signals from multiple cytokines: IL‐1, IL‐23, IL‐6 and TGF‐β,transforming growth factor, that can promote Th17 development and induce a Th17 response which promotes intestinal muscle hypercontractility that drives worm expulsion. TGFβ-activation by dendritic cells yields this Th17 induction and intestinal contractility and facilitates the expulsion of the parasite Trichinella spiralis in mice. This unique immune response of intestinal helminth expulsion beyond that of classical Th2 driven immunity, highlights the importance of IL-17 in parasitic disease. Th17 protection against parasites is very broad spectrum extending to Th17 cells’ providing robust protection against Trypanosoma cruzi, the intracellular protozoan parasite that causes Chagas disease. Parasites that establish long term chronic infections suppress Th17 immunity by modulation of antigen-specific CD4+ T responses. This is seen in human infection with the worm parasite Strongyloides stercoralis https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4546867/pdf/nihms-704134.pdf. Th17 cells of infected people showed significantly decreased responses upon antigen-stimulation, but following treatment, significantly increased the antigen-specific responses of Th17 cells. Th17 cells produce pro-inflammatory cytokines, including IL-17A, IL-17F, and IL-22. This cytokine production not only promotes accumulation of immune cells, such as macrophages, neutrophils and lymphocytes, at inflammatory sites, but also can cause collateral tissue damage. Other Th17 cells can negatively regulate immune responses by secreting immunosuppressive factors, such as IL-10 as noted in the response of children to COVID. Th17 cells are required for vaccine-induced protection against pulmonary infection with the pathogenic fungi Coccidioides posadasii, Histoplasma capsulatum, and Blastomyces dermatitidis, fungal pathogens causing systemic mycoses in humans. IL-17 is required for neutrophil and macrophage recruitment to the lungs. This balance is evidently what helps dispose of or suppress parasites and perhaps SARS-CoV-2 virus, or, if out of balance, severe acute or chronic persistent long hauler pathologies https://www.thermofisher.com/us/en/home/life-science/cell-analysis/cell-analysis-learning-center/immunology-at-work/t-helper-17-cell-overview.html. Some in vitro experiments suggest a benefit from Vitamin D because of its effects on Th17 cells. These cells are characterized by the chemokine receptor CCR6, RORC expression, and production of IL-17A, IFNγ, and TNFα. Using rheumatoid arthritis (RA) as a model of autoimmune disease, investigators demonstrated that pro-inflammatory memory CCR6+ Th cells can switch into anti-inflammatory cells by treating them with the active vitamin D metabolite 1,25(OH)2D3. Memory CCR6+ Th cells were sorted from healthy controls or treatment-naïve patients with early rheumatoid arthritis (RA) and cultured with or without 1,25(OH)2D3. Vitamin D3 inhibited pro-inflammatory cytokine production, IL-17A, IL-17F, IL-22 and IFNγ, in memory CCR6+ Th cells from both healthy controls and RA patients. This inhibition was accompanied by induction of anti-inflammatory factors, IL-10 and CTLA4 https://www.frontiersin.org/articles/10.3389/fimmu.2019.01504/full. Perhaps, this approach provides a means to test the hypothesis that Th17 memory cells are the root cause of long haulers. Also, antioxidants may help because the pro-inflammatory cytokines enhance the production of reactive oxygen species which are mediators of the anti-parasitic effector mechanism and collateral pathology. These benefits remain to be seen.
The anti-parasitic immune response leading to long haul and neurological disease has gained further support in a new paper showing the involvement of the cytokine CCL11, eosinophil chemotactic protein and eotaxin-1 (https://www.biorxiv.org/content/10.1101/2022.01.07.475453v1.full.pdf).
A prophet is not a soothsayer. Prophets are interpreters of the past, now and future. They see through the fog with clarity that is obvious to them and frustrating because of their lack of understanding of others inability to see. They are compelled, no driven, to tell what they see, even to the detriment of themselves and those they love. They have but one measure, the truth, to tell even if they would rather not. It is a Hand of what is Greater than themselves that leads, pushes, compells the way forward. Voices that cannot be silenced until they are spoken, even to the end. My book “Type B Cytochromes: Sensors and Switches”, the past, this blog, the now, “The Black Dragon Trilogy”, the vision, the dreams dreamt of the future. The last, the alternatives and options mapped out on the plain of space and time to be chosen with inevitable outcomes determined by the path chosen. “All those moments lost in time”, if ignored. Professionally dead but still alive.
This analysis is based on past experience and studies applicable to SARS-CoV-2, and the Omicron variant in particular. I still maintain that SARS-CoV-2 is an animal virus, a generalist, and opportunist with an imposed human bias. It has kept its options to infect and be maintained in animal species other than humans. Humans have just provided a profound opportunity for viral amplification and transmission with travel, global contact, disregard for sanitary precautions, socioeconomic disparity (poor vaccine distribution and preferential access to life saving treatments), and political interference (positive and negative influence). Omicron can be viewed as the natural evolutionary progression of the virus under these circumstances. Recent data has shown the first indications that Omicron is following an animal coronavirus pattern that I have described in several earlier posts. The confusion in the press and the debate amongst the scientific community over Omicron being more transmissible (clearly) and less pathogenic (awaiting more data) is an unclear relationship, if any connection at all, between pathogenicity (morbidity and mortality) and transmissibility. Transmissibility seems to follow a logical course of higher transmissibility leading to greater incidence and prevalence of a variant like Omicron, but it has its limitations. Transmissibility is not linear but asymptotic in is evolution. Too much transmissibility and vulnerable hosts become harder too find; too little and the virus infectivity dies out with distance between and immunity of hosts. An inhibition of immunity by the virus leads to greater viral production and lower infectious dose, but too much and the virus spreads throughout a host’s tissues that leads to incapacitation (limited mobility for viral spread) or lethality (eliminating a viral host for replication and spread); too much or too quick induction of immunity and not enough virus is available for transmission. These are the tensions pulling on virus mutations, governing its evolution.
Omicron has, in a preliminary study, shown a preference for infecting human upper respiratory tissue over lung tissue in culture. The omicron variant multiplies about 70 times faster inside human respiratory tract tissue than the delta variant does, according to a University of Hong Kong report (https://www.med.hku.hk/en/news/press/20211215-omicron-sars-cov-2-infection?utm_medium=social&utm_source=twitter&utm_campaign=press_release). This is supported by the fact that, in the U.S., cases caused by the Omicron variant jumped seven times in a week, from 0.4% to 2.9% total cases, according to Centers for Disease Control and Prevention estimates. The infection incidence is approaching 13% of cases in the region including New York and New Jersey. This is close to the prevalence of other coronaviruses in animal populations at any given time (10-15%). The preponderance in the upper respiratory tract (including bronchi) assures large amounts of virus will be expelled with coughs and sneezes and will most likely take hold in exposed susceptible people. Localized immunosuppression in these tissues before recovery is more than adequate to rapidly reproduce and provide time to spread the virus. No increase in pathogenicity is necessary.
However, a shift from preference for receptors deep in the lungs to those of the upper respiratory tract assuring more likely human to human transmission has been seen before in influenza. Avian influenza prefers deeper receptors in the human respiratory system and is more pathogenic. When it reassorts with other strains like those of pigs and humans, it becomes more transmissible in these species, mostly less pathogenic, but not always and without assurance of such a result. So no assurance of Omicron’s decrease in pathogenicity.
The increase in lethality of an infectious entity is often indifferent to transmissibility, especially if it is quick and a living host is not required to spread the agent. Sometimes the dead are a greater source of transmissible agent than the living and the agent is thus selected for lethality as it mutates or against attenuation that would allow recovery and elimination of the infectious form. This situation describes anthrax that is transmitted through spores that form upon death and dismemberment of the host. Even Ebola, until recently, was most likely to be transmitted from person to person by preparation of the dead for burial. Today, not just the dead and dying transmit it but also the recovered through chronic infection and sexual transmission. Its nature has changed as it has moved from being an East African sporadically occurring zoonoses to an endemic urban virus in West Africa. SAR-CoV-2, like other animal coronaviruses, is not so infectiously persistent in the environment, but rather spreads through constantly maintained susceptible populations and by acute and chronic viral shedders (in animals, mostly by the GI tract, yet to be fully demonstrated in human hosts infected with adapted coronaviruses). Time will tell if SARS-CoV-2, Omicron in particular, follows this well tread coronavirus path.
Did Omicron come out of animals? Sequences shared with coronaviruses in rats (https://media.nature.com/original/magazine-assets/d41586-022-00215-2/d41586-022-00215-2.pdf). Spreading to hamsters then back to humans (https://deliverypdf.ssrn.com/delivery.php?ID=905122026003114127079123119001002108070000006036012087096100017005026012108069005085117079006123024016028096075124024095120029035039092080082014103069087050015051047119025019073007018096068101116122057113095048023013018003005127004003074071116075102028010112004123113020012112075020103113022&EXT=pdf&INDEX=TRUE).
Isn’t it time for a totally new approach that is both specific and versatile? An approach that can be applied immediately before an emerging infectious disease goes pandemic? A means to “out evolve” a virus or antibiotic resistant bacteria or other microbe before it escapes its origin ? Yes, Nanobes . “I’ve seen things you people wouldn’t believe….all those moments lost in time like tears in the rain”.

{kind=link}