
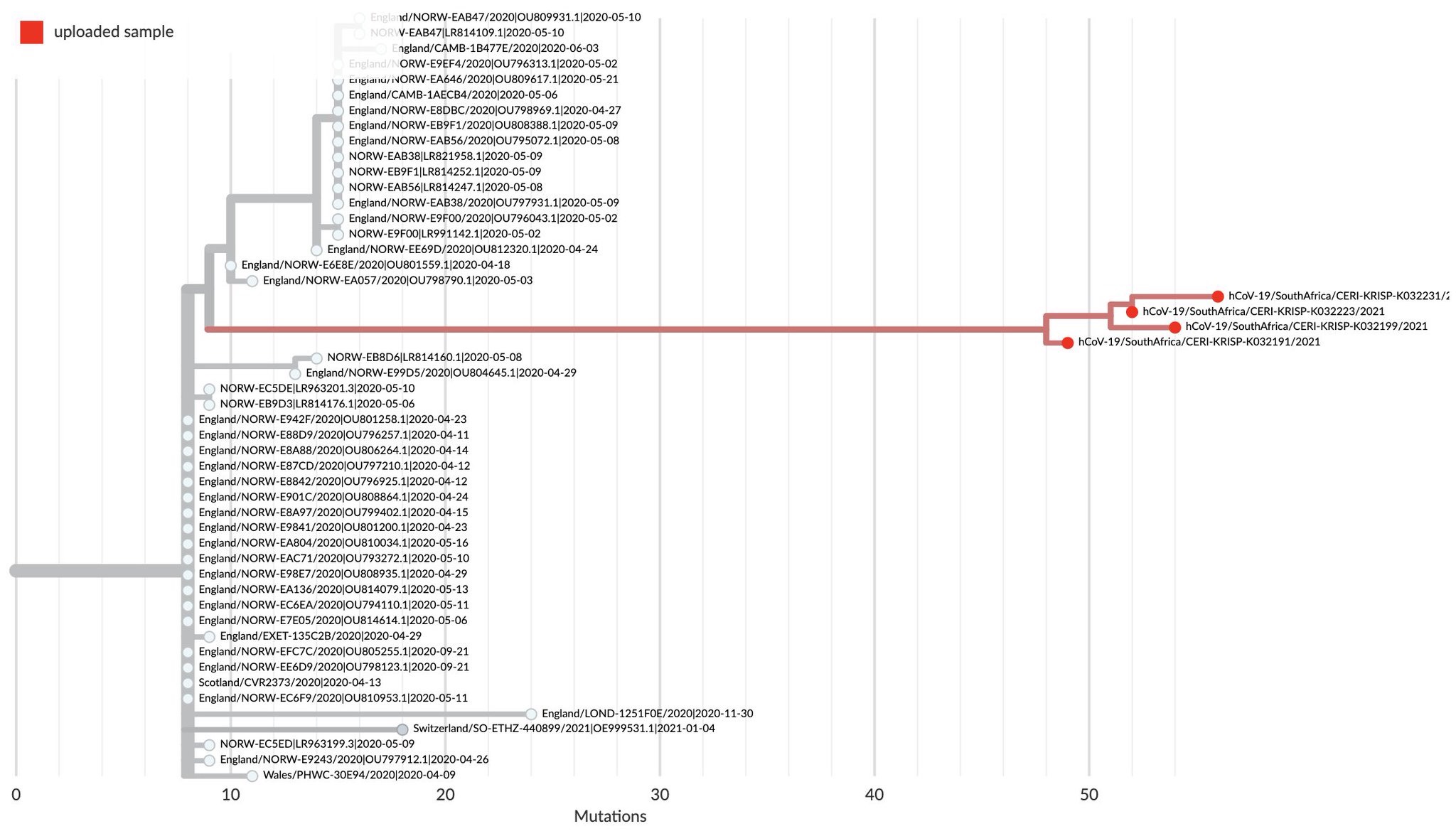
Recently, SARS-CoV-2, COVID, has shown that it has more surprises for us. The following diagram is based on the comparison of all the genomes of SARS-CoV-2 isolates grouped into related variants. The South African recent isolate variant (red lines) did not evolve from other current variants. The 91 genomes from Omicron viruses (@GISAID) were from specimens collected between Nov 11 and Nov 23 in Botswana, South Africa and Hong Kong. On 26 November, the World Health Organization (WHO) designated SARS-CoV-2 variant B.1.1.529, as a variant of concern and named it Omicron, on advice of scientists in the WHO’s Technical Advisory Group on SARS-CoV-2 Virus Evolution. Omicron was added to WHO list of current variants of concern: Delta, Alpha, Beta and Gamma. The Omicron variant has a high number of mutations especially in the spike protein. The extremely long red branch (>1 year) below indicates an extended period of circulation in a highly localized geographic area with poor genomic surveillance (not in South Africa proper but some contiguous or connected area by travel) or continual evolution in a chronically infected individual before spilling back into the population. It is not likely an animal source, as some have suggested, but has a peculiarity of one coronavirus, feline infectious peritonitis virus, in particular, that has been observed for many years and in another, originally zoonotic virus, that has been maintained in a slow but enduring pandemic, HIV.
The sources of this diagram are https://twitter.com/trvrb/status/1464353224417325066?s=21 and https://www.pango.network/.
For these changes to occur in such isolation, mutations forced by natural selection in a small number of hosts or in a single host, there must be one or more mechanisms of immune evasion and survival of the host(s) to allow for the time for these mutations to occur and to select for survival of the virus. How could one get Omicron variant ? Two CoVs could infect the same cell at once and share genetic material to make a new virus (homologous recombination). HIV generates mutations frequently, even within the same individual, because of the sequence mistakes made by reverse transcriptase, which converts the RNA to DNA, which is, in turn, inserted into the host genome from whence it is expressed as new virus. Even though coronaviruses have a proof reading RNA dependent RNA polymerase, they still make mistakes in replication, and mutations are also produced in the viral RNA templates by the active oxygen and nitrogen compounds produced by inflammatory cells which produce chemical changes in the RNA nucleotides which alter replicated sequences. The viral selection process is driven by the host immune system against the frequently changing protein structure, eliminating the variants for which it is specific and leaving behind the evading ones to enter new host cells and replicate. The anti-parasite immunity described in earlier posts may also be, at least in part, responsible in allowing the SARS-CoV-2 time to mutate and escape the immunity in a single host. This is seen in such parasitic diseases as African Sleeping Sickness (trypanosomiasis) and malaria, and may even produce a stalemate with the host called premunition, infectious immunity ( https://www.frontiersin.org/articles/10.3389/fimmu.2019.02738/full). It appears SARS-CoV-2 has chosen to enhance anti-parasite immunity like that used by the hosts to control parasitic worm, pathogenic protozoan and fungal infestations and infections. This response often controls the number of parasites to a tolerable, but not immediately lethal, level and prevents further infestation (process premunition), but does not totally eliminate the parasite. But is there any precedent for this in other coronaviruses in animals?
Cats get an enteric coronavirus which has little or no signs, but, in certain young cats, it becomes disseminated, causing peritonitis with lethality, usually 100%. Cell-mediated immunity provides an effective immune response that resolves the infection in the enteric, intestinal form. If it does not, a strong humoral response kicks in and selects for a more pathogenic form of the virus which infects and replicates in macrophages https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7112361/pdf/main.pdf. Also, autoantibodies form. There seems to be genetic predisposition toward this resulting in peritonitis https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2819880/. Peritonitis pathology involves severe systemic inflammatory damage of serosal membranes and widespread pyogranulomatous lesions in the lungs, liver, lymph tissue, and brain. The clinical finding of hypergamma-globulinemia-associated feline infectious peritonitis is indicative of over production of antibody against an antigen which cannot be cleared, allowing time for viral mutations that allow the virus to escape elimination. Therefore, like COVID-19, the feline coronavirus virus disease has this dichotomy, based on viral dissemination and autoantibodies. The right antigen for the right vaccine must be selected to prevent such adverse effects.
SARS-CoV-2, continues to evolve by mutation and selection toward being more efficient at infection and transmission within close, tight social groups but falling off quickly when vaccination and moderate barriers, like masks and good ventilation, and social distancing are implemented.
Vaccination does NOT guarantee protection from infection by Delta, Omicron, or any new variant or transient release of virus from asymptomatic vaccinated individuals. Vaccination is NOT for elimination of all possible virus but to reduce infection level below the point of symptoms of disease in immunized people (varies from person to person somewhat, but is more likely to be overcome with higher circulating viral loads). It is the circulating of more infectious particles over and over so there can be accumulation and increased probability of developing more mutants, therefore, variants, that is problematic. Omicron is just SARS-CoV-2 testing the perimeter for weaknesses.
The first Omicron case has arrived in the US in California in a person returning from South Africa Nov 22. Fully vaccinated, this person has displayed mild symptoms, is in quarantine, and all contacts tested have been negative so far (CDC).
